Localized Fibrosing Mediastinitis Causing Pulmonary Infarction: A Case Report
- Affiliations
-
- 1Department of Radiology, Ajou University School of Medicine, Suwon, Korea. sunnahn@ajou.ac.kr
- 2Department of Pathology, Ajou University School of Medicine, Suwon, Korea.
- KMID: 2164819
- DOI: http://doi.org/10.3348/jksr.2016.74.6.403
Abstract
- A 44-year-old female patient visited our emergency room for hemoptysis and refractory chest wall pain of 2 months duration. She had no history of smoking or other medical conditions. Chest CT scan showed homogenously enhancing soft tissue mass without calcification at the left pulmonary hilum. Encasing and compression of the left lower pulmonary artery by the mass had resulted in pulmonary infarction in the left lower lobe. Laboratory tests for tuberculosis, fungus, and vasculitis were all negative. The patient underwent surgical biopsy and resection of infarcted left lower lobe that was histopathologically confirmed as fibrosing mediastinitis. Herein, we reported a rare case of surgically confirmed and treated localized fibrosing mediastinitis causing pulmonary infarction.
MeSH Terms
Figure
-
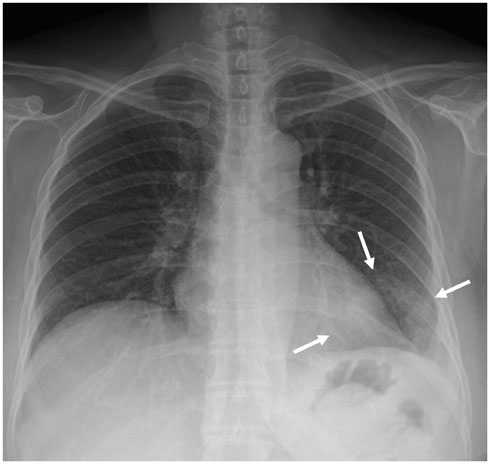
Fig. 1 Plain chest radiograph shows patchy increased opacity in left lower lung zone (arrows) and small amount of left pleural effusion.
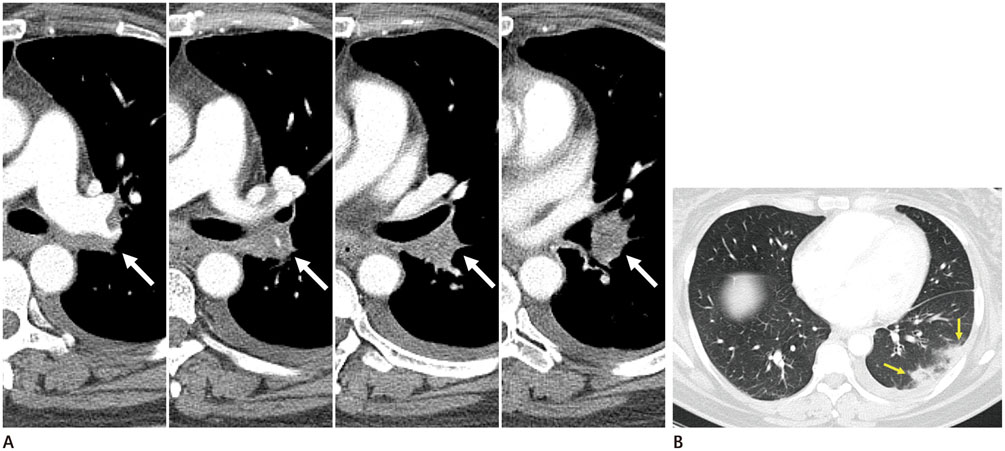
Fig. 2 Representative CT images of localized fibrosing mediastintis. A. Preoperative post-contrast chest CT demonstrates mediastinal soft tissue mass extending into left hilar region and encasing left lower pulmonary artery, causing severe stenosis or occlusion (white arrows). B. Multifocal wedge shaped consolidations with surrounding ground glass attenuation at subpleural area of left lower lobe suggesting pulmonary infarctions (yellow arrows).
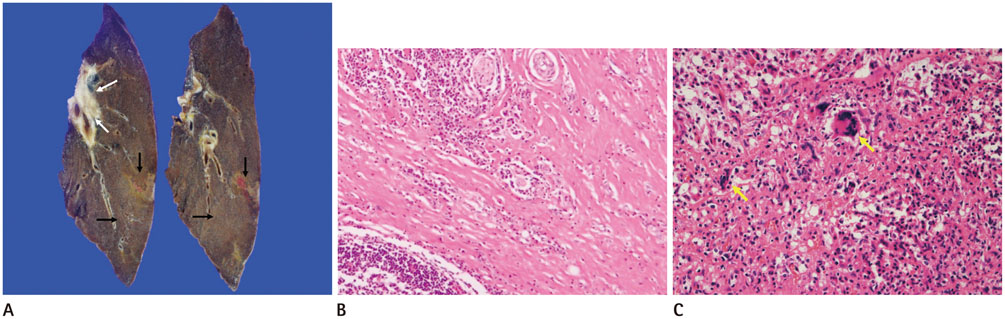
Fig. 3 Gross and microscopic specimens of localized fibrosing mediastintis. A. Photograph of cut surface of resected specimen demonstrates dense whitish fibrous tissue (white arrows) in left pulmonary hilum along the bronchovascular bundle with peripheral pulmonary infarctions (black arrows). B. High-power photomicrograph (original magnification, × 100, hematoxylin-eosin stain) of peripheral lung demonstrates extensive dense fibrosis. C. High-power photomicrograph (original magnification, × 100, hematoxylin-eosin stain) of left pulmonary hilum shows granulomatous inflammation (yellow arrows) with necrosis.
Reference
-
1. Schowengerdt CG, Suyemoto R, Main FB. Granulomatous and fibrous mediastinitis. A review and analysis of 180 cases. J Thorac Cardiovasc Surg. 1969; 57:365–379.2. Kittredge RD, Nash AD. The many facets of sclerosing fibrosis. Am J Roentgenol Radium Ther Nucl Med. 1974; 122:288–298.3. Devaraj A, Griffin N, Nicholson AG, Padley SP. Computed tomography findings in fibrosing mediastinitis. Clin Radiol. 2007; 62:781–786.4. Parish JM, Rosenow EC 3rd. Mediastinal granuloma and mediastinal fibrosis. Semin Respir Crit Care Med. 2002; 23:135–143.5. Loyd JE, Tillman BF, Atkinson JB, Des Prez RM. Mediastinal fibrosis complicating histoplasmosis. Medicine (Baltimore). 1988; 67:295–310.6. Rossi SE, McAdams HP, Rosado-de-Christenson ML, Franks TJ, Galvin JR. Fibrosing mediastinitis. Radiographics. 2001; 21:737–757.7. Goodwin RA, Nickell JA, Des Prez RM. Mediastinal fibrosis complicating healed primary histoplasmosis and tuberculosis. Medicine (Baltimore). 1972; 51:227–246.8. McNeeley MF, Chung JH, Bhalla S, Godwin JD. Imaging of granulomatous fibrosing mediastinitis. AJR Am J Roentgenol. 2012; 199:319–327.9. Peikert T, Colby TV, Midthun DE, Pairolero PC, Edell ES, Schroeder DR, et al. Fibrosing mediastinitis: clinical presentation, therapeutic outcomes, and adaptive immune response. Medicine (Baltimore). 2011; 90:412–423.10. Dunn EJ, Ulicny KS Jr, Wright CB, Gottesman L. Surgical implications of sclerosing mediastinitis. A report of six cases and review of the literature. Chest. 1990; 97:338–346.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Pulmonary Hypertension with Percutaneous Stenting of Pulmonary Artery in Fibrosing Mediastinitis
- Fibrosing Mediastinits Causing Obstruction of Left Lower Lobar Bronchus: A Pediatric Case Report
- Idiopathic Fibrosing Mediastinitis Causing Pulmonary Hypertension with Improvement by Steroid Treatment
- Fibrosing Mediastinitis: a Rare Cause of Unilateral Absent Lung Perfusion on a V/Q Scan
- Two Cases of Fibrosing Mediastinitis Caused by Tuberculosis
