A root submergence technique for pontic site development in fixed dental prostheses in the maxillary anterior esthetic zone
- Affiliations
-
- 1Department of Prosthodontics & Dental Research Institute, Seoul National University School of Dentistry, Seoul, Korea. proshan@snu.ac.kr
- 2Department of General Dentistry, Boston University School of Dental Medicine, Boston, MA, USA.
- KMID: 2164344
- DOI: http://doi.org/10.5051/jpis.2015.45.4.152
Abstract
- PURPOSE
This case report discusses the effect of a root submergence technique on preserving the periodontal tissue at the pontic site of fixed dental prostheses in the maxillary anterior aesthetic zone.
METHODS
Teeth with less than ideal structural support for fixed retainer abutments were decoronated at the crestal bone level. After soft tissue closure, the final fixed dental prostheses were placed with the pontics over the submerged root area. Radiographic and clinical observations at the pontic sites were documented.
RESULTS
The submerged roots at the pontic sites preserved the surrounding periodontium without any periapical pathology. The gingival contour at the pontic site was maintained in harmony with those of the adjacent teeth, as well as the overall form of the arch.
CONCLUSIONS
The results of this clinical report indicate that a root submergence technique can be successfully applied in pontic site development with fixed dental prostheses, especially in the maxillary anterior esthetic zone.
Keyword
Figure
-

Figure 1 Radiographic images and a clinical photograph of the patient in Case 1. (A) Intraoral radiographic image at the patient's first visit. (B) Intraoral radiographic image three months after the removal of an existing restoration and endodontic treatment on the maxillary right lateral incisor. (C) Intraoral radiographic image two years after the delivery of a final fixed dental prosthesis. (D) Clinical photograph two years after the delivery.
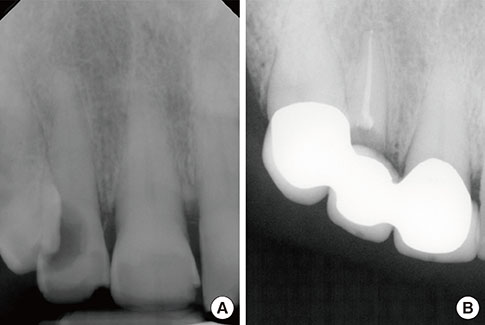
Figure 2 Radiographic images of the patient in Case 2. (A) At the first visit, a cavity extended to the crestal bone level on the distal surface of the maxillary right lateral incisor. (B) No pathology was noted three months after the final restoration.
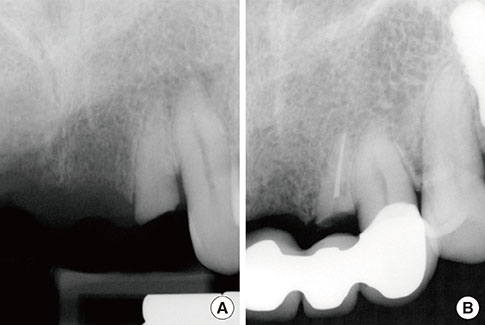
Figure 3 Radiographic images of the patient in Case 3. (A) A maxillary left lateral incisor tooth was fractured and pulpal tissue was exposed. (B) No pathologic changes were noted 24 months after the final restoration.
Cited by 1 articles
-
Endodontic management of central incisor associated with large periapical lesion and fused supernumerary root: a conservative approach
Gautam P. Badole, Pratima R. Shenoi, Ameya Parlikar
Restor Dent Endod. 2018;43(4):. doi: 10.5395/rde.2018.43.e44.
Reference
-
1. Ishida Y, Fujimoto K, Higaki N, Goto T, Ichikawa T. End points and assessments in esthetic dental treatment. J Prosthodont Res. 2015; Forthcoming.
Article2. Fradeani M. Esthetic analysis: a systematic approach to prosthetic treatment. Chicago (IL): Quintessence Publishing;2004.3. Atwood DA, Coy WA. Clinical, cephalometric, and densitometric study of reduction of residual ridges. J Prosthet Dent. 1971; 26:280–295.
Article4. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003; 23:313–323.5. Jambhekar S, Kernen F, Bidra AS. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: a systematic review of randomized controlled clinical trials. J Prosthet Dent. 2015; 113:371–382.
Article6. Avila-Ortiz G, Elangovan S, Kramer KW, Blanchette D, Dawson DV. Effect of alveolar ridge preservation after tooth extraction: a systematic review and meta-analysis. J Dent Res. 2014; 93:950–958.
Article7. Morjaria KR, Wilson R, Palmer RM. Bone healing after tooth extraction with or without an intervention: a systematic review of randomized controlled trials. Clin Implant Dent Relat Res. 2014; 16:1–20.
Article8. Casey DM, Lauciello FR. A review of the submerged-root concept. J Prosthet Dent. 1980; 43:128–132.
Article9. O'Neal RB, Gound T, Levin MP, del Rio CE. Submergence of roots for alveolar bone preservation. I. Endodontically treated roots. Oral Surg Oral Med Oral Pathol. 1978; 45:803–810.10. Gound T, O'Neal RB, del Rio CE, Levin MP. Submergence of roots for alveolar bone preservation. II. Reimplanted endodontically treated roots. Oral Surg Oral Med Oral Pathol. 1978; 46:114–122.11. Welker WA, Jividen GJ, Kramer DC. Preventive prosthodontics--mucosal coverage of roots. J Prosthet Dent. 1978; 40:619–621.
Article12. Harper KA. Submerging an endodontically treated root to preserve the alveolar ridge under a bridge--a case report. Dent Update. 2002; 29:200–203.13. Salama M, Ishikawa T, Salama H, Funato A, Garber D. Advantages of the root submergence technique for pontic site development in esthetic implant therapy. Int J Periodontics Restorative Dent. 2007; 27:521–527.14. Wong KM, Chneh CM, Ang CW. Modified root submergence technique for multiple implant-supported maxillary anterior restorations in a patient with thin gingival biotype: a clinical report. J Prosthet Dent. 2012; 107:349–352.
Article15. Çomut A, Mehra M, Saito H. Pontic site development with a root submergence technique for a screw-retained prosthesis in the anterior maxilla. J Prosthet Dent. 2013; 110:337–343.
Article16. Garver DG, Fenster RK. Vital root retention in humans: a final report. J Prosthet Dent. 1980; 43:368–373.
Article17. von Wowern N, Winther S. Submergence of roots for alveolar ridge preservation. A failure (4-year follow-up study). Int J Oral Surg. 1981; 10:247–250.18. Gongloff RK. Vital root retention. A 5-year experience. Int J Oral Maxillofac Surg. 1986; 15:33–38.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pontic site development with an implant submergence technique for unaesthetic implant in the anterior maxilla
- The esthetic prosthodontic treatments in maxillary anterior area, considering the gingival margin
- Accurate transfer of gingival morphology to definitive prostheses using temporary prostheses
- Fiber-reinforced composite resin bridges: an alternative method to treat root-fractured teeth
- Esthetic restoration in continuous maxillary anterior area using immediate implant placement: A case report
