Korean J Urol.
2015 Jun;56(6):429-434. 10.4111/kju.2015.56.6.429.
The clinical significance of a second transurethral resection for T1 high-grade bladder cancer: Results of a prospective study
- Affiliations
-
- 1Department of Urology, Korea University Ansan Hospital, Ansan, Korea. jaeyoungpark@korea.ac.kr
- 2Department of Urology, Korea University Anam Hospital, Seoul, Korea.
- 3Department of Urology, Korea University College of Medicine, Seoul, Korea.
- 4Department of Urology, Korea University Guro Hospital, Seoul, Korea.
- KMID: 2160582
- DOI: http://doi.org/10.4111/kju.2015.56.6.429
Abstract
- PURPOSE
This study was designed to estimate the value of a second transurethral resection of bladder tumor (TURBT) procedure in patients with initially diagnosed T1 high-grade bladder cancer.
MATERIALS AND METHODS
Between August 2009 and January 2013, a total of 29 patients with T1 high-grade bladder cancer prospectively underwent a second TURBT procedure. Evaluation included the presence of previously undetected residual tumor, changes to histopathological staging or grading, and tumor location. Recurrence-free and progression-free survival curves were generated to compare the prognosis between the groups with and without residual lesions by use of the Kaplan-Meier method.
RESULTS
Of 29 patients, 22 patients (75.9%) had residual disease after the second TURBT. Staging was as follows: no tumor, 7 (24.1%); Ta, 5 (17.2%); T1, 6 (20.7%); Tis, 6 (20.7%); Ta+Tis, 1 (3.4%); T1+Tis, 1 (3.4%); and > or =T2, 3 (10.3%). The muscle layer was included in the surgical specimen after the initial TURBT in 24 patients (82.7%). In three patients whose cancer was upstaged to pT2 after the second TURBT, the initial surgical specimen contained the muscle layer. In the group with residual lesions, the 3-year recurrence-free survival and 3-year progression-free survival rates were 50% and 66.9%, respectively, whereas these rates were 68.6% and 68.6%, respectively, in the group without residual lesions. This difference was not statistically significant.
CONCLUSIONS
Initial TURBT does not seem to be enough to control T1 high-grade bladder cancer. Therefore, a routine second TURBT procedure should be recommended in patients with T1 high-grade bladder cancer to accomplish adequate tumor resection and to identify patients who may need to undergo prompt cystectomy.
MeSH Terms
Figure
-
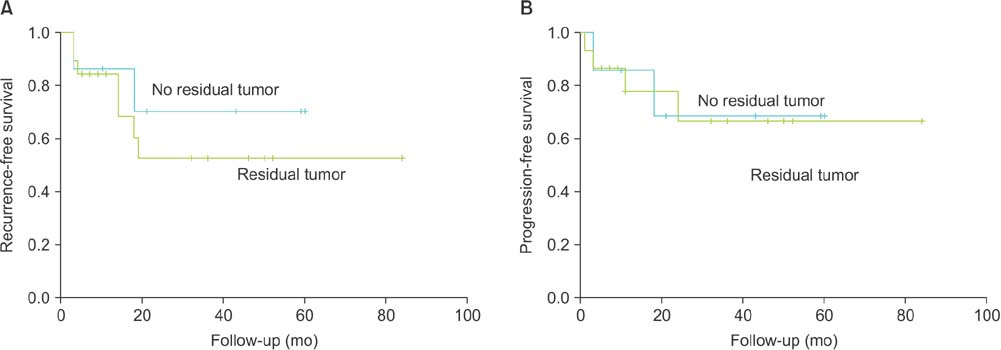
Fig. 1 (A) Kaplan-Meier curves of recurrence-free survival (RFS) in patients with residual tumor (green) and without residual tumor (blue) at the second transurethral resection of bladder tumor (TURBT). Three-year RFS was 68.6% and 50%, respectively (p=0.5). (B) Kaplan-Meier curves of progression-free survival (PFS) in patients with residual tumor (green) and without residual tumor (blue) at the second TURBT. Three-year PFS was 66.9% and 68.6%, respectively (p=0.976).
Reference
-
1. Divrik RT, Sahin AF, Yildirim U, Altok M, Zorlu F. Impact of routine second transurethral resection on the long-term outcome of patients with newly diagnosed pT1 urothelial carcinoma with respect to recurrence, progression rate, and diseasespecific survival: a prospective randomised clinical trial. Eur Urol. 2010; 58:185–190.2. Babjuk M, Oosterlinck W, Sylvester R, Kaasinen E, Bohle A, Palou-Redorta J, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder. Eur Urol. 2008; 54:303–314.3. Clark P, Agarwal N, Biagioli M. NCCN clinical practice guidelines in oncology: bladder cancer. Fort Washington (PA): National Comprehensive Cancer Network;2013.4. Babjuk M. Second resection for non-muscle-invasive bladder carcinoma: current role and future perspectives. Eur Urol. 2010; 58:191–192.5. Ali MH, Ismail IY, Eltobgy A, Gobeish A. Evaluation of second-look transurethral resection in restaging of patients with nonmuscle-invasive bladder cancer. J Endourol. 2010; 24:2047–2050.6. Herr HW. Restaging transurethral resection of high risk superficial bladder cancer improves the initial response to bacillus Calmette-Guerin therapy. J Urol. 2005; 174:2134–2137.7. Katumalla FS, Devasia A, Kumar R, Kumar S, Chacko N, Kekre N. Second transurethral resection in T1G3 bladder tumors - Selectively avoidable? Indian J Urol. 2011; 27:176–179.8. Lazica DA, Bottcher S, Degener S, von Rundstedt FC, Brandt AS, Roth S, et al. T1 high-grade bladder cancer - value of second operation with prognostuic parameters of first operation: analysis of 167 cases. Aktuelle Urol. 2013; 44:124–128.9. Takaoka E, Matsui Y, Inoue T, Miyazaki J, Nakashima M, Kimura T, et al. Risk factors for intravesical recurrence in patients with high-grade T1 bladder cancer in the second TUR era. Jpn J Clin Oncol. 2013; 43:404–409.10. Yucel M, Hatipoglu NK, Atakanli C, Yalcinkaya S, Dedekarginoglu G, Saracoglu U, et al. Is repeat transurethral resection effective and necessary in patients with T1 bladder carcinoma? Urol Int. 2010; 85:276–280.11. Babjuk M, Burger M, Zigeuner R, Shariat SF, van Rhijn BW, Comperat E, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2013. Eur Urol. 2013; 64:639–653.12. Han KS, Joung JY, Cho KS, Seo HK, Chung J, Park WS, et al. Results of repeated transurethral resection for a second opinion in patients referred for nonmuscle invasive bladder cancer: the referral cancer center experience and review of the literature. J Endourol. 2008; 22:2699–2704.13. Dalbagni G, Herr HW, Reuter VE. Impact of a second transurethral resection on the staging of T1 bladder cancer. Urology. 2002; 60:822–824.14. Brauers A, Buettner R, Jakse G. Second resection and prognosis of primary high risk superficial bladder cancer: is cystectomy often too early? J Urol. 2001; 165:808–810.15. Novara G, Ficarra V. Does routine second transurethral resection affect the long-term outcome of patients with T1 bladder cancer? Why a flawed randomized controlled trial cannot address the issue. Eur Urol. 2010; 58:193–194.16. Schips L, Augustin H, Zigeuner RE, Galle G, Habermann H, Trummer H, et al. Is repeated transurethral resection justified in patients with newly diagnosed superficial bladder cancer? Urology. 2002; 59:220–223.17. Zurkirchen MA, Sulser T, Gaspert A, Hauri D. Second transurethral resection of superficial transitional cell carcinoma of the bladder: a must even for experienced urologists? Urol Int. 2004; 72:99–102.18. Sivalingam S, Probert JL, Schwaibold H. The role of repeat transurethral resection in the management of high-risk superficial transitional cell bladder cancer. BJU Int. 2005; 96:759–762.19. Holmang S. High-grade non-muscle-invasive bladder cancer: is re-resection necessary in all patients before intravesical bacillus Calmette-Guérin treatment? Scand J Urol. 2013; 47:363–369.20. Oosterlinck W, Solsona E, van der Meijden AP, Sylvester R, Bohle A, Rintala E, et al. EAU guidelines on diagnosis and treatment of upper urinary tract transitional cell carcinoma. Eur Urol. 2004; 46:147–154.21. Dutta SC, Smith JA Jr, Shappell SB, Coffey CS, Chang SS, Cookson MS. Clinical under staging of high risk nonmuscle invasive urothelial carcinoma treated with radical cystectomy. J Urol. 2001; 166:490–493.22. Chen WM, Cheng CL, Yang CR, Chung V. Surgical tip to prevent bladder perforation during transurethral resection of bladder tumors. Urology. 2008; 72:667–668.23. Jocham D, Witjes F, Wagner S, Zeylemaker B, van Moorselaar J, Grimm MO, et al. Improved detection and treatment of bladder cancer using hexaminolevulinate imaging: a prospective, phase III multicenter study. J Urol. 2005; 174:862–866.24. Babjuk M, Oosterlinck W, Sylvester R, Kaasinen E, Bohle A, Palou-Redorta J, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder, the 2011 update. Eur Urol. 2011; 59:997–1008.25. Kulkarni GS, Hakenberg OW, Gschwend JE, Thalmann G, Kassouf W, Kamat A, et al. An updated critical analysis of the treatment strategy for newly diagnosed high-grade T1 (previously T1G3) bladder cancer. Eur Urol. 2010; 57:60–70.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- How do we manage high-grade T1 bladder cancer? Conservative or aggressive therapy?
- Recurrence According to Grade after BCG Intravesical Therapy in Stage T1 Bladder Cancer
- A Clinical Efficacy of Intravesical Bacillus Calmette-Guerin Therapy of Stage T1 Bladder Cancer
- Intraoperative ventilation and hemodynamic change due to bladder perforation during transurethral resection of a bladder tumor: A case report
- Predicting Progression and Survival in Korean Patients with High Grade T1 Bladder Cancer Using EORTC Risk Tables
