Korean J Neurotrauma.
2013 Oct;9(2):146-149. 10.13004/kjnt.2013.9.2.146.
Tracheoesophageal Fistula: A Fatal Complication of Endotracheal Intubation
- Affiliations
-
- 1Department of Neurosurgery, Daejeon St. Mary's Hospital, College of Medicine (Nursing), The Catholic University of Korea, Daejeon, Korea. yijinseok@hanmail.net
- KMID: 2156118
- DOI: http://doi.org/10.13004/kjnt.2013.9.2.146
Abstract
- Tracheoesophageal fistula (TEF) is a rare disease which develops as a result of congenital or acquired causes. We report on two TEF female stroke patients with associated endotracheal intubation. Endotracheal intubation was kept for 13-14 days because of decreased mentality by intracranial hemorrhage. Recurrent pneumonia was a predominant symptom. Computed tomography and bronchoscopy were used to diagnose TEF. Both patients expired by sepsis and recurrent pneumonia before definite TEF treatment. The excessive dilatation of the cuff balloon of the endotracheal tube was considered one of the main causes of TEF. Prevention is most important and early treatment is required in this fatal disease.
MeSH Terms
Figure
-

FIGURE 1. Chest radiogram checked 3 days after admission shows the excessively dilated cuff of the endotracheal intubation tube.
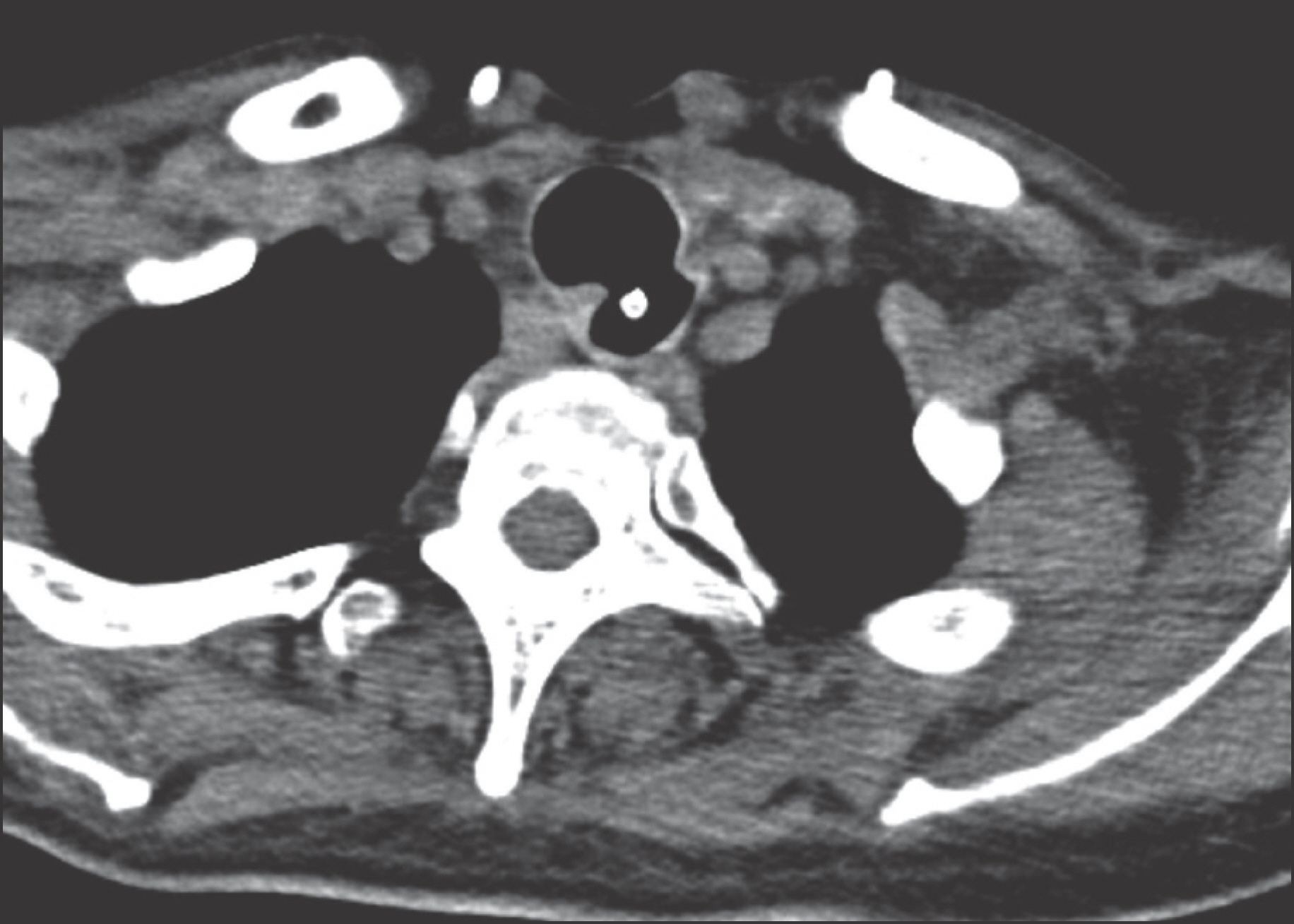
FIGURE 2. Tracheoesophageal fistula is seen between the esophagus and the trachea on neck computed tomography in case 1. The white dot is the Levin tube in the esophagus.
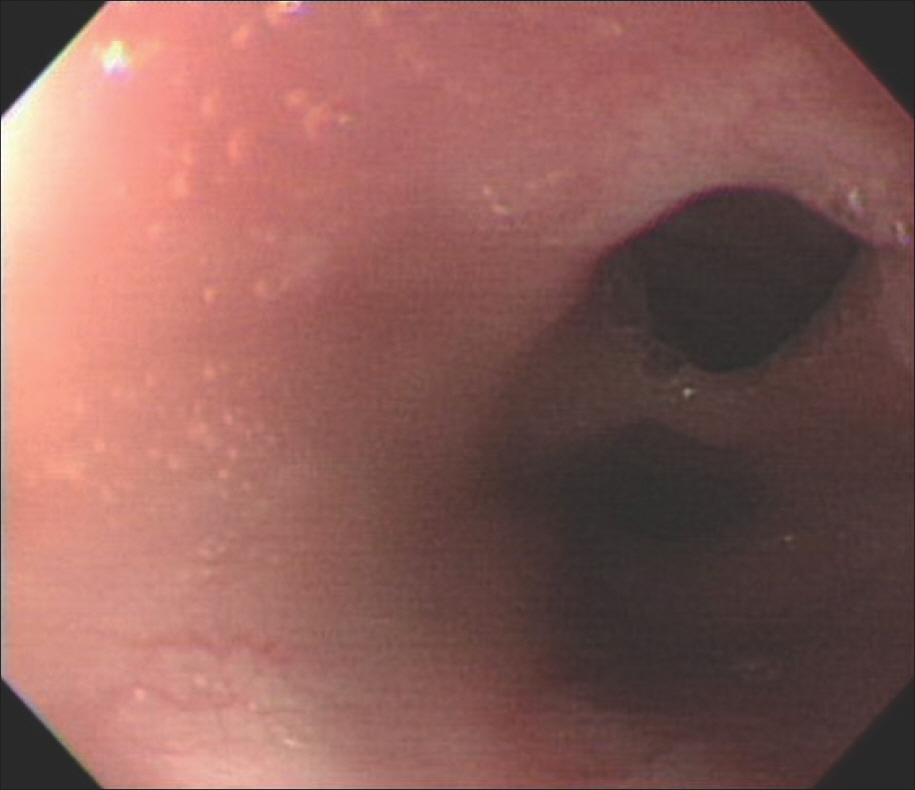
FIGURE 3. Tracheoesophageal fistula observed at 18 cm from incisor under endoscopic view in case 1. The upper lumen is the trachea and the lower lumen is the esophagus.
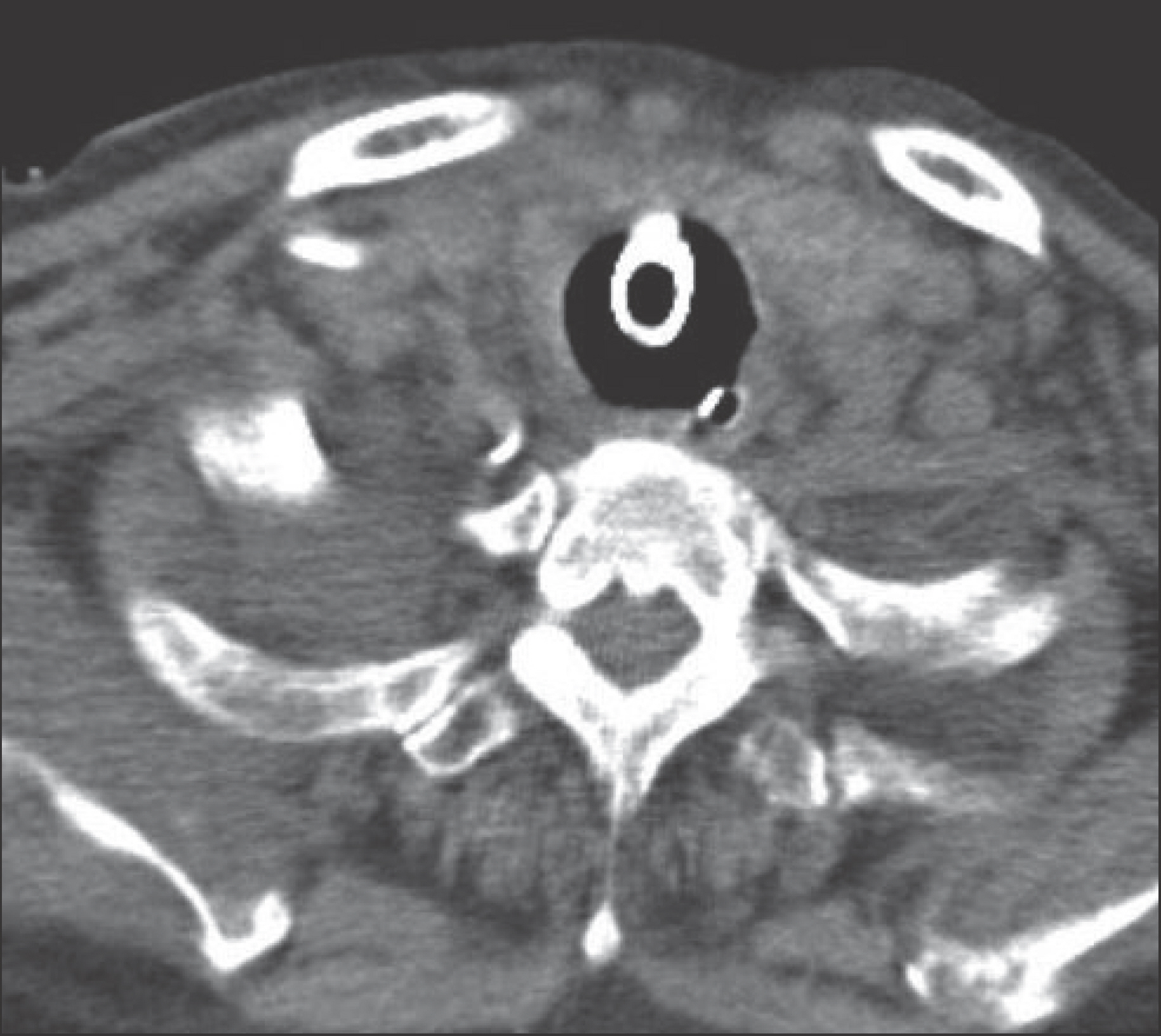
FIGURE 4. Tracheoesophageal fistula is seen between the esophagus and the trachea on neck computed tomography in case 2. The white dot is the Levin tube in the esophagus.

FIGURE 5. Universal cuff pressure instrument of the intubation tube.
Reference
-
References
1. Black RJ. Congenital tracheo-oesophageal fistula in the adult. Thorax. 37:61–63. 1982.
Article2. Chahine AA, Newman KD. Surgery for congenital lesions of the esophagus in Sellke FW, del Nido PJ, Swanson SJ (eds): Sabiston & Spencer Surgery of the Chest, ed 7. Philadelphia: Elsevier Saunders, pp567–581;2005.3. Grillo HC. Development of tracheal surgery: a historical review. Part 2: Treatment of tracheal diseases. Ann Thorac Surg. 75:1039–1047. 2003.4. Kim HM, No JK, Cho YS, Kim HJ. Application of a loss of resistance syringe for obtaining the adequate cuff pressures of endotracheal intubated patients in an emergency department. J Korean Soc Emerg Med. 23:769–775. 2012.5. Macchiarini P, Verhoye JP, Chapelier A, Fadel E, Dartevelle P. Evaluation and outcome of different surgical techniques for pos-tintubation tracheoesophageal fistulas. J Thorac Cardiovasc Surg. 119:268–276. 2000.
Article6. Shanmuganathan K, Mirvis SE. Imaging diagnosis of nonaortic thoracic injury. Radiol Clin North Am. 37:533–551. vi,. 1999.
Article7. Spalding AR, Burney DP, Richie RE. Acquired benign bronchoesophageal fistulas in the adult. Ann Thorac Surg. 28:378–383. 1979.
Article8. Thomas AN. Management of tracheoesophageal fistula caused by cuffed tracheal tubes. Am J Surg. 124:181–189. 1972.
Article9. Tsai FC, Lin PJ, Wu YC, Chang CH. Traumatic aortic arch transection with supracarinal tracheoesophageal fistula: case report. J Trauma. 46:951–953. 1999.10. Tu HN, Saidi N, Leiutaud T, Bensaid S, Menival V, Duvaldestin P. Nitrous oxide increases endotracheal cuff pressure and the incidence of tracheal lesions in anesthetized patients. Anesth Analg. 89:187–190. 1999.
Article11. Wychulis AR, Ellis FH Jr, Andersen HA. Acquired nonmalignant esophagotracheobronchial fistula. Report of 36 cases. JAMA. 196:117–122. 1966.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tracheoesophageal Fistula as a Complication after Endotracheal Intubation: A Case Report
- Two Cases of Postintubation Tracheoesophageal Fistula in Patients with a History of Tracheostomy: Case Report
- Tracheoesophageal Fistula Due to Endotracheal Intubation; a case Report of Requiring Tracheal Reconstruction
- Acquired Tracheoesophageal Fistula Observed during Anesthetic Induction: A case report
- Repair of Tracheoesophageal Fistula under Laryngeal Microsurgery Approach: Case Report and Literature Review
