Persistent Truncus Arteriosus with Aortic Dominance in Female Adult Patient
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea.
- 2Department of Pediatrics, Kyungpook National University School of Medicine, Daegu, Korea. kimyhmd@knu.ac.kr
- KMID: 2135404
- DOI: http://doi.org/10.4250/jcu.2015.23.1.32
Abstract
- Persistent truncus arteriosus categories associated with different natural histories and various surgical approaches were reported. Although pulmonary overflow and severe heart failure are common, some patients who have hypoplastic pulmonary artery systems may show lesser symptoms of heart failure and remain in relatively stable condition. We experienced a 33-year-old woman with uncorrected type II persistent truncus arteriosus who presented with cyanosis rather than congestive heart failure, and are presenting her images.
Keyword
MeSH Terms
Figure
-
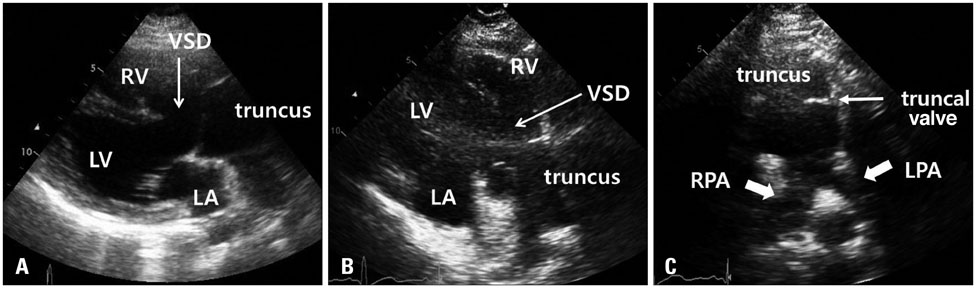
Fig. 1 The images of parasternal long and short axis view of transthoracic echocardiography. A parasternal long axis view showed an overriding non-restrictive ventricular septal defect (VSD) supplied by both ventricles (A), and a single great vessel overriding both ventricles from the base of the heart (B). A parasternal short axis view showed absence of the main pulmonary arterial trunk, and adjacent right and left pulmonary arteries (PAs) that arose separately from the dorsal aspect of the common trunk (C). The size of the origins of the right and left PAs in bifurcation from the main PA were 12 mm (Z-score = -1.3) and 8 mm (Z-score = -5.7), respectively. RV: right ventricle, LV: left ventricle, LA: left atrium, RPA: right pulmonary artery, LPA: left pulmonary artery.
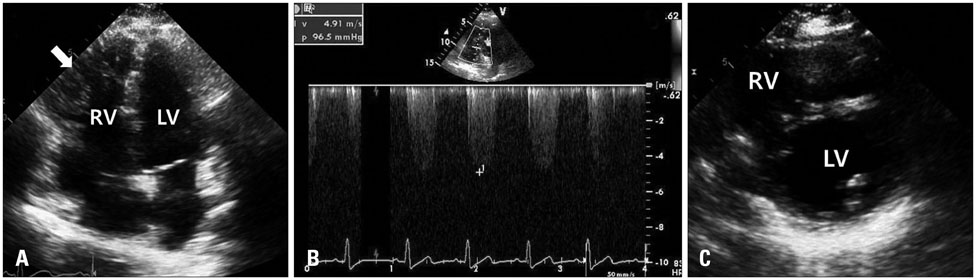
Fig. 2 An apical 4 chamber view revealed a hypertrophied right ventricle (A). The systolic flow velocity of TR was 4.9 m/s (B) and interventricular septum during the systolic phase was flat, systolic D shaped LV (C). RV: right ventricle, LV: left ventricle.
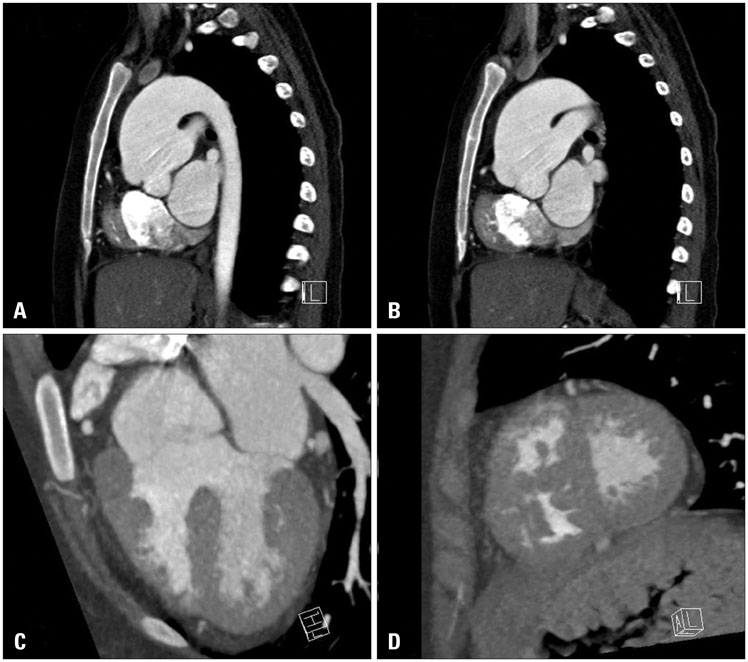
Fig. 3 Electrocardiogram-gated multidetector computed tomography showed pulmonary arteries arising separately from the dorsal aspect of the common trunk (A and B), overriding non-restrictive ventricular septal defect supplied by both ventricles (C), hypertrophied right ventricle and flat interventricular septum (D).
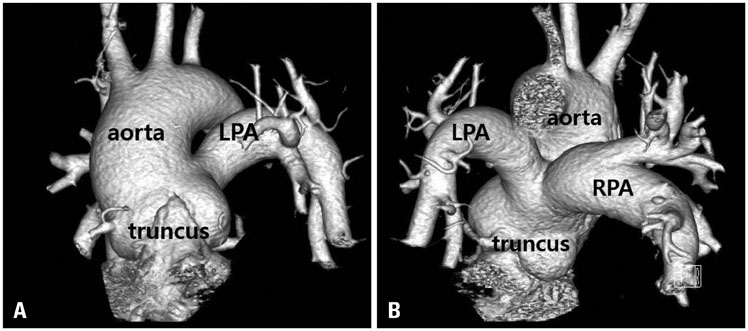
Fig. 4 Two images acquired from three dimensional reconstruction of electrocardiogram-gated multidetector computed tomography showed that two pulmonary arteries arose from the posterior aspect of the truncus separately but close to each other. Antero-lateral aspect (A) and dorsal aspect (B). RPA: right pulmonary artery, LPA: left pulmonary artery.
Reference
-
1. Slavik Z, Keeton BR, Salmon AP, Sutherland GR, Fong LV, Monro JL. Persistent truncus arteriosus operated during infancy: long-term follow-up. Pediatr Cardiol. 1994; 15:112–115.2. Bodí V, Insa L, Sanchis J, Ibáñez M, Losada A, Chorro FJ. Persistent truncus arteriosus type 4 with survival to the age of 54 years. Int J Cardiol. 2002; 82:75–77.3. Hicken P, Evans D, Heath D. Persistent truncus arteriosus with survival to the age of 38 years. Br Heart J. 1966; 28:284–286.4. Guenther F, Frydrychowicz A, Bode C, Geibel A. Cardiovascular flashlight. Persistent truncus arteriosus: a rare finding in adults. Eur Heart J. 2009; 30:1154.5. Espínola-Zavaleta N, Muñoz-Castellanos L, González-Flores R, Kuri-Nivón M. [Common truncus arteriosus in adults]. Arch Cardiol Mex. 2008; 78:210–216.6. Russell HM, Jacobs ML, Anderson RH, Mavroudis C, Spicer D, Corcrain E, Backer CL. A simplified categorization for common arterial trunk. J Thorac Cardiovasc Surg. 2011; 141:645–653.7. Marcelletti C, McGoon DC, Mair DD. The natural history of truncus arteriosus. Circulation. 1976; 54:108–111.8. Boris JR. Primary care management of patients with common arterial trunk and transposition of the great arteries. Cardiol Young. 2012; 22:761–767.
