Hemorrhagic Recurrence in Diffuse Astrocytoma without Malignant Transformation
- Affiliations
-
- 1Department of Neurosurgery, Eulji University Hospital, College of Medicine, Eulji University, Daejeon, Korea. nsksm@eulji.ac.kr
- KMID: 2134283
- DOI: http://doi.org/10.14791/btrt.2014.2.2.119
Abstract
- Although uncommon, hemorrhage can be a complication of low grade glioma with an unfavorable prognosis such as transformation to higher grade glioma. To our knowledge, hemorrhagic recurrence of World Health Organization Grade II, diffuse astrocytoma without malignant transformation has not been reported. Thus, we report a case of diffuse astrocytoma with hemorrhagic recurrence without malignant transformation. The patient had undergone craniotomy and tumor removal 7 years previously. Annual follow-up MRIs had shown evidence of slow tumor recurrence. With the sudden onset of seizure, the patient was diagnosed as hemorrhagic recurrence and underwent second tumor removal highly suspecting malignant change into higher grade glioma. Histopathology confirmed diffuse astrocytoma without malignant changes. As the patient's postoperative condition was excellent, we plan to withhold chemotherapy and radiation therapy for use as a later treatment option.
Keyword
MeSH Terms
Figure
-
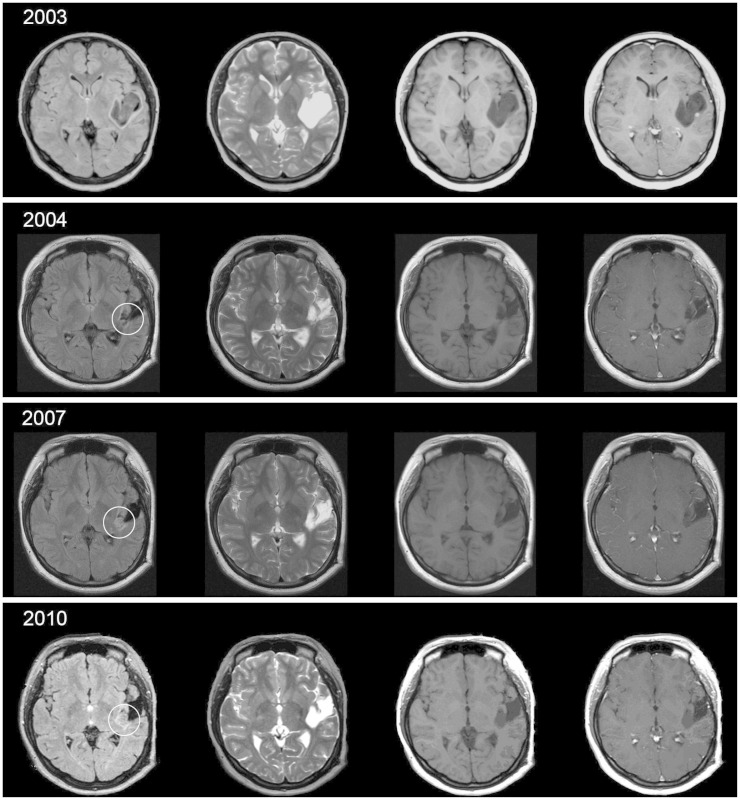
Fig. 1 Series of annual MRI follow-up from immediate post operation since 2003 to 2010, before the hemorrhagic event. In series of MRI fluid attenuation inversion recovery, circled lesion shows slow changes in most medial portion of the tumor boundary.
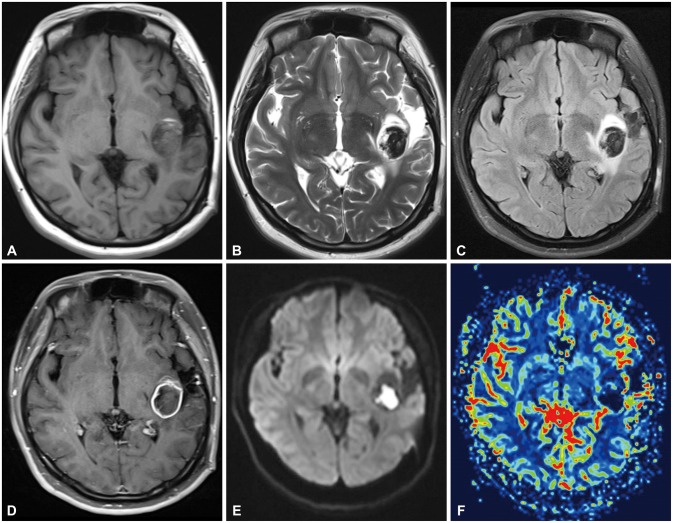
Fig. 2 Initial MRI after dysarthria and headache. A and B: The images show T1-, T2-weighted image of acute onset hemorrhage with surrounding gliotic changes from the previous operation. C and D: Flair and T1 enhancement image shows peripheral thin rim enhancing lesion about 32×28×24 mm at the left perisylvian posterior insula, subinsula, posterior external capsule white matter area, with surrounding mild edema. E and F: MR diffusion and regional cerebral blood volume (rCBV) image of the patient. Note that increase in rCBV from the peripheral enhancing thin rim of the Lt. perisylvian superior temporal hemorrhagic lesion.
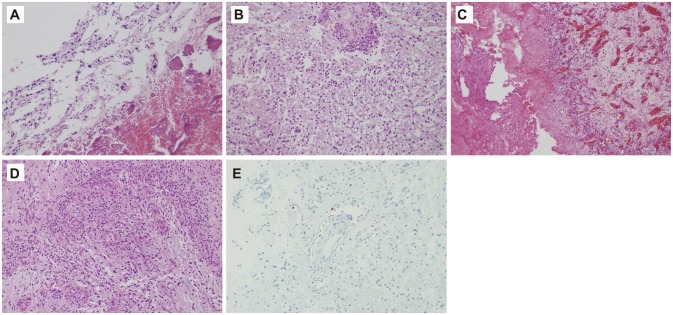
Fig. 3 Histopathology. A: Histology of 1st operation (hematoxylin-eosin stain, ×200).Tumor cells with mild nuclear atypia are present in fibrillary background, diagnosed as diffuse astrocytoma. B: Histology of main lesion of 2nd operation (hematoxylin-eosin stain, ×200). The neoplastic astrocytes with occasional nuclear atypia and glomeruloid vessels are present in the background of a loosely structured or microcystic tumor matrix, diagnosed as astrocytoma. C: Main lesion 2nd operation (hematoxylin-eosin stain, ×100). Evidence of hemorrhage and vascular proliferation of the main lesion is present. D: Main lesion 2nd operation (hematoxylin-eosin stain, ×200). Neovascularization is identified along the edge of tumor periphery. E: There is 1-2% stain of tumor cells in Ki-67 immunohistochemical staining (×200).
Reference
-
1. Della Puppa A, Zustovich F, Gardiman M, Manara R, Cecchin D, Scienza R. Haemorrhagic presentation of low-grade glioma in adults. Acta Neurochir (Wien). 2007; 149:1151–1155. discussion 1155. PMID: 17676407.
Article2. Rees J, Watt H, Jäger HR, et al. Volumes and growth rates of untreated adult low-grade gliomas indicate risk of early malignant transformation. Eur J Radiol. 2009; 72:54–64. PMID: 18632238.
Article3. Shafqat S, Hedley-Whyte ET, Henson JW. Age-dependent rate of anaplastic transformation in low-grade astrocytoma. Neurology. 1999; 52:867–869. PMID: 10078745.
Article4. Combs SE, Ahmadi R, Schulz-Ertner D, Thilmann C, Debus J. Recurrent low-grade gliomas: the role of fractionated stereotactic re-irradiation. J Neurooncol. 2005; 71:319–323. PMID: 15735924.
Article5. Licata B, Turazzi S. Bleeding cerebral neoplasms with symptomatic hematoma. J Neurosurg Sci. 2003; 47:201–210. discussion 210. PMID: 14978474.6. Marton E, Feletti A, Orvieto E, Longatti P. Malignant progression in pleomorphic xanthoastrocytoma: personal experience and review of the literature. J Neurol Sci. 2007; 252:144–153. PMID: 17189643.
Article7. White JB, Piepgras DG, Scheithauer BW, Parisi JE. Rate of spontaneous hemorrhage in histologically proven cases of pilocytic astrocytoma. J Neurosurg. 2008; 108:223–226. PMID: 18240915.
Article8. Shibahara I, Kanamori M, Kumabe T, et al. Hemorrhagic onset of pilocytic astrocytoma and pilomyxoid astrocytoma. Brain Tumor Pathol. 2009; 26:1–5. PMID: 19408090.
Article9. Mishra KK, Puri DR, Missett BT, et al. The role of up-front radiation therapy for incompletely resected pediatric WHO grade II low-grade gliomas. Neuro Oncol. 2006; 8:166–174. PMID: 16495375.10. Brada M, Viviers L, Abson C, et al. Phase II study of primary temozolomide chemotherapy in patients with WHO grade II gliomas. Ann Oncol. 2003; 14:1715–1721. PMID: 14630674.
Article11. Karim AB, Afra D, Cornu P, et al. Randomized trial on the efficacy of radiotherapy for cerebral low-grade glioma in the adult: European Organization for Research and Treatment of Cancer Study 22845 with the Medical Research Council study BRO4: an interim analysis. Int J Radiat Oncol Biol Phys. 2002; 52:316–324. PMID: 11872276.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Malignant Transformation of Juvenile Pilocytic Astrocytoma with Neurofibromatosis Type 1
- Early Recurrence of a Lateral Ventricle Meningioma with Malignant Transformation
- Early High-Grade Transformation of IDH-Mutant Central Nervous System WHO Grade 2 Astrocytoma: A Case Report
- Intracranial Metastases of Cervical Intramedullary Low-Grade Astrocytoma without Malignant Transformation in Adult
- Transdural Extension of Malignant Astrocytoma
