Obliteration of Radical Cavities and Total Reconstruction Procedure Without Staging After Canal Wall Down Mastoidectomy: Long-term Results
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan. borrong_huang@hotmail.com
- KMID: 2117517
- DOI: http://doi.org/10.3342/ceo.2015.8.3.230
Abstract
OBJECTIVES
We evaluate the long-term surgical and hearing results using a canal wall down mastoidectomy technique followed by cavities obliteration, canal wall reconstruction and ossiculoplasty without staging.
METHODS
A total of 44 patients between January 2002 and October 2009 were selected and 27 of them were revision cases. Preoperative and postoperative pure tone average (PTA) and air-bone gap (ABG) were assessed and compared 1 and 4 years after surgery.
RESULTS
The middle ear was well healed and aerated in 40 patients (90.9%) and the tympanic membrane was intact in 42 patients (95.5%). Recurrent cholesteatoma was found on postoperative follow-up in two of the revision patients (7.4%) but none in the primary patients. Seven patients were found to have partial canal bone absorption, but revision surgery was not required. Over 86.4% of all cases were water resistant. Long-lasting improvement and/or preservation of hearing, with maintenance of PTA-ABG closure in 63.7% of all cases within 20 dB, were obtained.
CONCLUSION
The efficacy of our technique after a canal wall down mastoidectomy is satisfactory, and the rate of complication is acceptably low. We believe that our technique could be a convenient method in disease control and providing an excellent basis for hearing restoration simultaneously.
Keyword
MeSH Terms
Figure
-
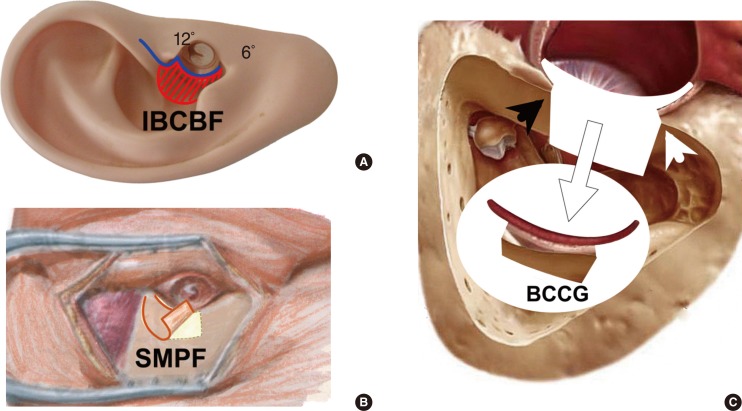
Fig. 1 Schematic figures of operating technique. (A) An endoaural incision was made as Heermann B incision. (B) A superiorly meatal pedicle flap (SMPF) about 15-mm width and 25- to 30-mm length was designed and elevated. (C) A free bone-connective tissue composite graft (BCCG, white arrow) was harvested (black arrowhead, anterior buttress; white arrowhead, posterior buttress). IBCBF, inferiorly based conchal bowl flap.
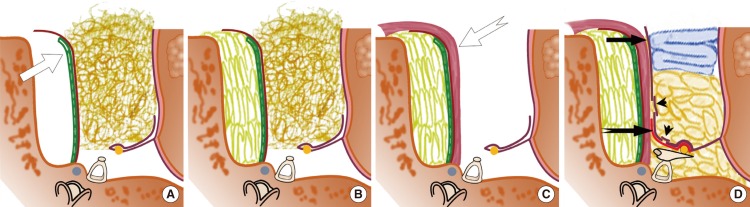
Fig. 2 Schematic figures of operating technique. (A) The posterior bone canal wall is reconstructed with the bone-connective tissue composite graft (white arrow). (B) The cavities are obliterated with bone chips and pâté, using the parallel overlapping stacking method. (C) The superiorly meatal pedicle flap (white bifid tail arrow) is shielded the surface of the obliterated cavity. (D) The ossicle chain and eardrum is reconstructed without staging (black arrow, inferiorly based conchal bowl flap; black bifid tail arrow, tympanomeatal flap; black arrowheads, split-thickness skin grafts).
Reference
-
1. Singh V, Atlas M. Obliteration of the persistently discharging mastoid cavity using the middle temporal artery flap. Otolaryngol Head Neck Surg. 2007; 9. 137(3):433–438. PMID: 17765771.
Article2. Gantz BJ, Wilkinson EP, Hansen MR. Canal wall reconstruction tympanomastoidectomy with mastoid obliteration. Laryngoscope. 2005; 10. 115(10):1734–1740. PMID: 16222186.
Article3. Gyo K, Sasaki Y, Hinohira Y, Yanagihara N. Residue of middle ear cholesteatoma after intact canal wall tympanoplasty: surgical findings at one year. Ann Otol Rhinol Laryngol. 1996; 8. 105(8):615–619. PMID: 8712631.
Article4. Wilson KF, Hoggan RN, Shelton C. Tympanoplasty with intact canal wall mastoidectomy for cholesteatoma: long-term surgical outcomes. Otolaryngol Head Neck Surg. 2013; 8. 149(2):292–295. PMID: 23674568.5. Wolfensberger M, Hilger PA, Hilger JA. Conchal bowl and postauricular flaps for reconstruction of the external auditory canal. Otolaryngol Head Neck Surg. 1983; 8. 91(4):404–406. PMID: 6415588.
Article6. Kim MB, Choi J, Lee JK, Park JY, Chu H, Cho YS, et al. Hearing outcomes according to the types of mastoidectomy: a comparison between canal wall up and canal wall down mastoidectomy. Clin Exp Otorhinolaryngol. 2010; 12. 3(4):203–206. PMID: 21217961.
Article7. Edfeldt L, StrOmbAck K, Kinnefors A, Rask-Andersen H. Surgical treatment of adult cholesteatoma: long-term follow-up using total reconstruction procedure without staging. Acta Otolaryngol. 2013; 1. 133(1):28–34. PMID: 23113656.
Article8. Roberson JB Jr, Mason TP, Stidham KR. Mastoid obliteration: autogenous cranial bone pAte reconstruction. Otol Neurotol. 2003; 3. 24(2):132–140. PMID: 12621322.9. McElveen JT Jr, Chung AT. Reversible canal wall down mastoidectomy for acquired cholesteatomas: preliminary results. Laryngoscope. 2003; 6. 113(6):1027–1033. PMID: 12782816.
Article10. Leatherman BD, Dornhoffer JL. The use of demineralized bone matrix for mastoid cavity obliteration. Otol Neurotol. 2004; 1. 25(1):22–25. PMID: 14724487.
Article11. Mahendran S, Yung MW. Mastoid obliteration with hydroxyapatite cement: the Ipswich experience. Otol Neurotol. 2004; 1. 25(1):19–21. PMID: 14724486.
Article12. Ramsey MJ, Merchant SN, McKenna MJ. Postauricular periosteal-pericranial flap for mastoid obliteration and canal wall down tympanomastoidectomy. Otol Neurotol. 2004; 11. 25(6):873–878. PMID: 15547414.
Article13. Takahashi H, Iwanaga T, Kaieda S, Fukuda T, Kumagami H, Takasaki K, et al. Mastoid obliteration combined with soft-wall reconstruction of posterior ear canal. Eur Arch Otorhinolaryngol. 2007; 8. 264(8):867–871. PMID: 17340129.
Article14. Linthicum FH Jr. The fate of mastoid obliteration tissue: a histopathological study. Laryngoscope. 2002; 10. 112(10):1777–1781. PMID: 12368614.
Article15. Black B. Mastoidectomy elimination: obliterate, reconstruct, or ablate? Am J Otol. 1998; 9. 19(5):551–557. PMID: 9752959.16. Grote JJ, van Blitterswijk CA. Reconstruction of the posterior auditory canal wall with a hydroxyapatite prosthesis. Ann Otol Rhinol Laryngol Suppl. 1986; Mar-Apr. 123:6–9. PMID: 3083756.
Article17. Clark MP, Bottrill I. SerenoCem-glass ionomeric granules: a 3-year follow-up assessment of their effectiveness in mastoid obliteration. Clin Otolaryngol. 2007; 8. 32(4):287–290. PMID: 17651273.18. Brown JS. A ten year statistical follow-up of 1142 consecutive cases of cholesteatoma: the closed vs. the open technique. Laryngoscope. 1982; 4. 92(4):390–396. PMID: 7070181.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Modified Canal Wall Down Mastoidectomy Without Meatoplasty
- Reconstruction of the Posterior Canal Wall with Mastoid Obliteration after Canal Wall Down Mastoidectomy
- Mastoid Obliteration with Bone Paste and Fat
- A Case of Repair of Retroauricular Skin Defect and Mastoid Cavity with Posterior Wall Reconstruction Using Tutoplast(R)(Allograft Cancellous Bone Chip) and Bone Dust after Canal Wall Down Mastoidectomy
- Mastoid Obliteration with Silicone Blocks after Canal Wall Down Mastoidectomy
