The Difference in Diagnostic Performance for Detection of Supraspinatus Tendon Tears by Adding Angled Oblique Sagittal Plane Image to the Routine Shoulder MRI
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Hospital, Seoul, Korea. reonora@schmc.ac.kr
- 2Department of Radiology, Soonchunhyang University Hospital, Bucheon, Korea.
- KMID: 2099892
- DOI: http://doi.org/10.13104/jksmrm.2014.18.2.157
Abstract
- PURPOSE
The purpose of this study is to determine whether adding an angled oblique sagittal plane to the routine shoulder MRI improves the diagnostic performance in the evaluation of supraspinatus tendon tears with arthroscopic correlation.
MATERIALS AND METHODS
The study included 121 patients who had a shoulder MRI followed by arthroscopy. Two radiologists separately evaluated the supraspinatus tendon for tears on shoulder MRI either with or without the angled oblique sagittal images. Arthroscopy was used as the reference standard. The sensitivity and specificity for diagnosing supraspinatus tendon tears were calculated and compared by using McNemar test. Interobserver and intertechnique variability in the interpretation of supraspinatus tendon tears were calculated as a kappa value.
RESULTS
Adding the angled oblique sagittal images to the standard shoulder MRI showed improvement in the sensitivity for diagnosing full-thickness supraspinatus tendon tears and also in the sensitivity, specificity and accuracy for the detection of partial-thickness tears. However, there was no statistically significant difference in all of them between with and without the angled set. Interobserver agreement was substantial to almost perfect and intertechnique agreement was moderate.
CONCLUSION
Adding an angled oblique sagittal plane image to the routine shoulder MRI showed no significantly different diagnostic performance in detecting the partial- and full-thickness supraspinatus tendon tears, compared to MRI without angled oblique sagittal plane.
MeSH Terms
Figure
-
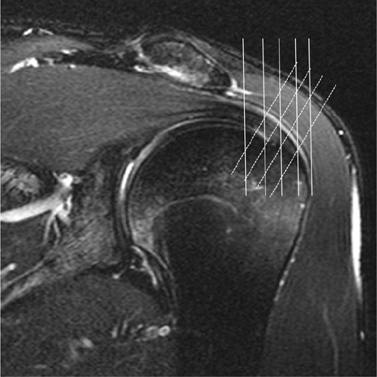
Fig. 1 Oblique coronal fat-suppressed fast spin-echo T2-weighted image (TR/TE, 4050/97) through the mid-glenoid fossa with the angled oblique sagittal image locations oriented perpendicular to the down-sloping lateral rotator cuff tendon (dashed lines).

Fig. 2 A 54-year-old women with a full-thickness supraspinatus tendon tear at arthroscopy. Oblique sagittal T2-weighted image (a) and oblique coronal fat-suppressed T2-weighted image (b) showed a focal area of increased signal (arrowheads) within the articular surface of the tendon. Angled oblique sagittal T2-weighted image showed linear high signal (arrowheads) extending from the articular to the bursal surface of the tendon (c). Arthroscopy confirmed the full-thickness supraspinatus tendon tear and repair was done (d).

Fig. 3 The false-positive partial-thickness tear of the supraspinatus tendon in 48-year-old women. Oblique sagittal T2-weighted image (a) and oblique coronal fat-suppressed T2-weighted image (b) showed a faint area of increased signal (arrow) within the bursal surface of the tendon. Angled oblique sagittal T2-weighted image also showed a faint increased signal (arrow) (c). This was scored as a partial-thickness tear by reader 1 and 2, however, there was impingement syndrome with no rotator cuff tear at arthroscopy (d).

Fig. 4 The false-negative partial-thickness tear of the supraspinatus tendon in 39-year-old man. Oblique sagittal T2-weighted image (a) and oblique coronal fat-suppressed T2-weighted image (b) showed intrasubstance with increased signal intensity (within the dashed line), which is lower than the signal intensity of the joint fluid. Angled oblique sagittal T2-weighted image showed a diffuse area of intermediate signal intensity (within the dashed line) (c). This patient was suggested with fraying of supraspinatus tendon with findings of underlying rotator cuff impingement at MRI by reader 1 and 2. However, articular view at arthroscopy showed the partialthickness tear at the articular surface of the supraspinatus tendon (arrow) (d).
Reference
-
1. Meislin RJ, Sperling JW, Stitik TP. Persistent shoulder pain: epidemiology, pathophysiology, and diagnosis. Am J Orthop (Belle Mead NJ). 2005; 34:5–9.2. Waldt S, Bruegel M, Mueller D, et al. Rotator cuff tears: assessment with MR arthrography in 275 patients with arthroscopic correlation. Eur Radiol. 2007; 17:491–498.3. Favard L, Bacle G, Berhouet J. Rotator cuff repair. Joint Bone Spine. 2007; 74:551–557.4. Neri BR, Chan KW, Kwon YW. Management of massive and irreparable rotator cuff tears. J Shoulder Elbow Surg. 2009; 18:808–818.5. Goergen SK, Bradley WG Jr, Liu J, et al. Improving the diagnostic accuracy of MR in the detection of infraspinatus tendon injuries. J Comput Assist Tomogr. 1996; 20:829–833.6. Tuite MJ, Asinger D, Orwin JF. Angled oblique sagittal MR imaging of rotator cuff tears: comparison with standard oblique sagittal images. Skeletal Radiol. 2001; 30:262–269.7. Reinus WR, Shady KL, Mirowitz SA, Totty WG. MR diagnosis of rotator cuff tears of the shoulder: value of using T2-weighted fat-saturated images. AJR Am J Roentgenol. 1995; 164:1451–1455.8. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33:159–174.9. Brox JI. Regional musculoskeletal conditions: shoulder pain. Best Pract Res Clin Rheumatol. 2003; 17:33–56.10. de Jesus JO, Parker L, Frangos AJ, Nazarian LN. Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: a meta-analysis. AJR Am J Roentgenol. 2009; 192:1701–1707.11. Dinnes J, Loveman E, McIntyre L, Waugh N. The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review. Health Technol Assess. 2003; 7:iii1–166.12. Wright T, Yoon C, Schmit BP. Shoulder MRI refinements: differentiation of rotator cuff tear from artifacts and tendonosis, and reassessment of normal findings. Semin Ultrasound CT MR. 2001; 22:383–395.13. Kijowski R, Farber JM, Medina J, Morrison W, Ying J, Buckwalter K. Comparison of fat-suppressed T2-weighted fast spin-echo sequence and modified STIR sequence in the evaluation of the rotator cuff tendon. AJR Am J Roentgenol. 2005; 185:371–378.14. Sahin-Akyar G, Miller TT, Staron RB, McCarthy DM, Feldman F. Gradient-echo versus fat-suppressed fast spin-echo MR imaging of rotator cuff tears. AJR Am J Roentgenol. 1998; 171:223–227.15. Singson RD, Hoang T, Dan S, Friedman M. MR evaluation of rotator cuff pathology using T2-weighted fast spin-echo technique with and without fat suppression. AJR Am J Roentgenol. 1996; 166:1061–1065.16. Fukuda H. The management of partial-thickness tears of the rotator cuff. J Bone Joint Surg Br. 2003; 85:3–11.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 16-Slice MDCT Arthrography of the Shoulder: Accuracy for Detection of Glenoid Labral and Rotator Cuff Tears
- Isokinetic Muscle Strength and Muscle Endurance by the Types and Size of Rotator Cuff Tear in Men
- Relationship of the Sagittal Extent of Rotator Cuff Tears to the Grade of Fatty Degeneration of the Rotator Cuff Muscles
- Diagnosis of Partial Thickness Tear of Supraspinatus Tendon Using Dynamic Ultrasonography Under Resisted Scaption Position
- The Test-Retest Reliability of Supraspinatus Cross-Sectional Area Measurement by Sonography
