High-resolution MR Imaging of Carotid Atherosclerotic Plaques
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yhchoe@skku.edu
- KMID: 2099843
- DOI: http://doi.org/10.13104/jksmrm.2012.16.2.97
Abstract
- High-resolution carotid MRI allows visualization of carotid atherosclerotic plaque characteristics. MRI serves as a noninvasive option for the detection of active plaque inflammation and intraplaque hemorrhage. Significant gains in signal-to-noise ratio and contrast-to-noise ratio can be obtained for carotid atheroma imaging at 3T compared with 1.5T. Normalized wall index or wall area on MRI has shown its efficacy in monitoring the response after medical therapy. T(2)* quantification in carotid plaques before and after the administration of ultrasmall superparamagnetic iron oxide particles shows difference in response to treatment according to drug doses. In conclusion, high-resolution MRI is useful in the diagnosis and monitoring of carotid atherosclerotic plaques prone to transient ischemic attack and stroke.
MeSH Terms
Figure
-
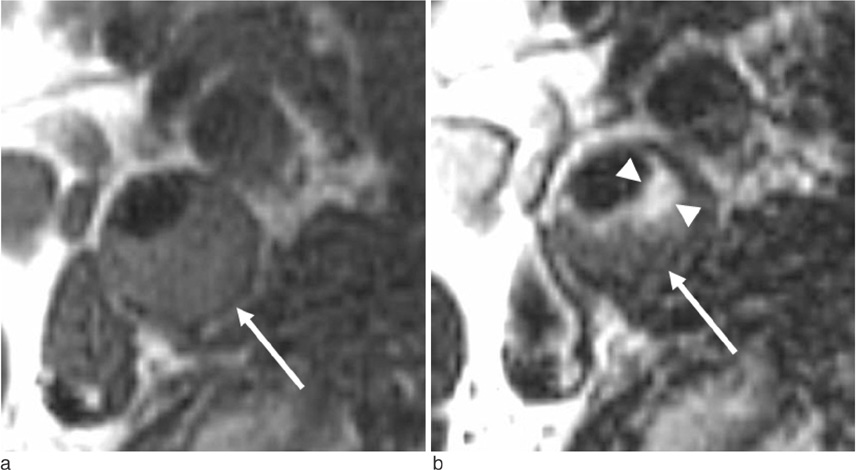
Fig. 1 Lipid-rich plaque. T1-weighted image (a) shows slightly increased signal intensity in the plaque (arrow). T2-weighted image shows a portion of bright signal intensity (arrowheads in the plaque which suggests the presence of fibrosis. The darker signal intensity in the plaque (arrow) implicates lipid-rich components.

Fig. 2 Hemorrhagic plaque in a 64-year-old male with vascular dementia. The plaque signal intensity is bright on a T1-weighted image (a), T1-weighted image with fat-saturation (b), and source image of time-of-flight MR angiography (c). On a maximum intensity projection image (d), there is a halo sign (arrow) due to intraplaque hemorrhage.
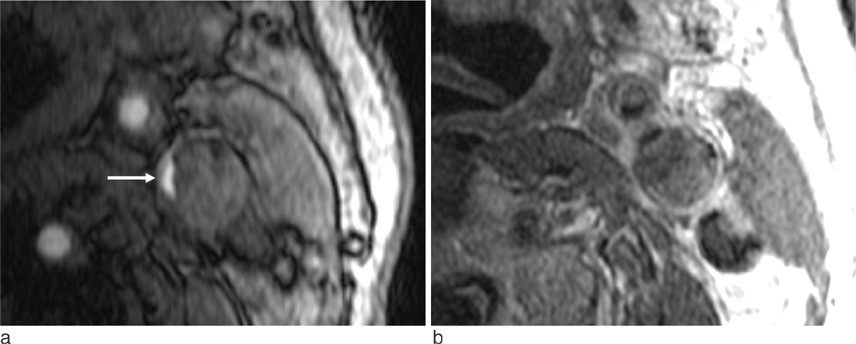
Fig. 3 Necrotic plaque in a 73-year-old male with stroke. a. A source image of time-of-flight MR angiography shows severe luminal narrowing (arrow) of the left internal carotid artery. b. contrast-enhanced T1-weighted MR image shows no significant enhancement in the plaque except the outer layers.

Fig. 4 Plaque regression after statin treatment in a 73-year-old male. a. T1-weighted image with fat-saturation at 1.5T shows an eccentric plaque in the left internal carotid artery. b. T1-weighted image with fat-saturation at 3T shows significant improvement in plaque thickness after 3-year low dose statin treatment.
Reference
-
1. Underhill HR, Yuan C. Carotid MRI: a tool for monitoring individual response to cardiovascular therapy? Expert Rev Cardiovasc Ther. 2011. 9:63–80.2. Hatsukami TS, Yuan C. MRI in the early identification and classification of high-risk atherosclerotic carotid plaques. Imaging Med. 2010. 2:63–75.3. Yim YJ, Choe YH, Ko Y, et al. High signal intensity halo around the carotid artery on maximum intensity projection images of time-of-flight MR angiography: a new sign for intraplaque hemorrhage. J Magn Reson Imaging. 2008. 27:1341–1346.4. Young VE, Patterson AJ, Tunnicliffe EM, et al. Signal-to-noise ratio increase in carotid atheroma MRI: a comparison of 1.5 and 3 T. Br J Radiol. 2012. 85:937–944.5. Mihai G, Winner MW, Raman SV, Rajagopalan S, Simonetti OP, Chung YC. Assessment of carotid stenosis using three-dimensional T2-weighted dark blood imaging: initial experience. J Magn Reson Imaging. 2012. 35:449–455.6. Costanzo P, Cleland JG, Atkin SL, Vassallo E, Perrone-Filardi P. Use of carotid intima-media thickness regression to guide therapy and management of cardiac risks. Curr Treat Options Cardiovasc Med. 2012. 14:50–56.7. Dong L, Wang J, Yarnykh VL, et al. Efficient flow suppressed MRI improves interscan reproducibility of carotid atherosclerosis plaque burden measurements. J Magn Reson Imaging. 2010. 32:452–458.8. Yang EY, Polsani VR, Washburn MJ, et al. Real-time co-registration using novel ultrasound technology: ex vivo validation and in vivo applications. J Am Soc Echocardiogr. 2011. 24:720–728.9. Duivenvoorden R, de Groot E, Elsen BM, et al. In vivo quantification of carotid artery wall dimensions: 3.0-Tesla MRI versus B-mode ultrasound imaging. Circ Cardiovasc Imaging. 2009. 2:235–242.10. Horie N, Morikawa M, Ishizaka S, et al. Assessment of carotid plaque stability based on the dynamic enhancement pattern in plaque components with multidetector CT angiography. Stroke. 2012. 43:393–398.11. Tartari S, Rizzati R, Righi R, et al. High-resolution MRI of carotid plaque with a neurovascular coil and contrast-enhanced MR angiography: one-stop shopping for the comprehensive assessment of carotid atherosclerosis. AJR Am J Roentgenol. 2011. 196:1164–1171.12. Kwee RM, van Oostenbrugge RJ, Hofstra L, et al. Identifying vulnerable carotid plaques by noninvasive imaging. Neurology. 2008. 70:2401–2409.13. Patterson AJ, Tang TY, Graves MJ, Muller KH, Gillard JH. In vivo carotid plaque MRI using quantitative T2* measurements with ultrasmall superparamagnetic iron oxide particles: a dose-response study to statin therapy. NMR Biomed. 2011. 24:89–95.14. Virani SS, Catellier DJ, Pompeii LA, et al. Relation of cholesterol and lipoprotein parameters with carotid artery plaque characteristics: the Atherosclerosis Risk in Communities (ARIC) carotid MRI study. Atherosclerosis. 2011. 219:596–602.15. Muller M, van der Graaf Y, Algra A, Hendrikse J, Mali WP, Geerlings MI. Carotid atherosclerosis and progression of brain atrophy: the SMART-MR study. Ann Neurol. 2011. 70:237–244.16. Ota H, Yu W, Underhill HR, et al. Hemorrhage and large lipid-rich necrotic cores are independently associated with thin or ruptured fibrous caps: an in vivo 3T MRI study. Arterioscler Thromb Vasc Biol. 2009. 29:1696–1701.17. Kurosaki Y, Yoshida K, Endo H, Chin M, Yamagata S. Association between carotid atherosclerosis plaque with high signal intensity on T1-weighted imaging and subsequent ipsilateral ischemic events. Neurosurgery. 2011. 68:62–67. discussion 67.18. Albuquerque LC, Narvaes LB, Maciel AA, et al. Intraplaque hemorrhage assessed by high-resolution magnetic resonance imaging and C-reactive protein in carotid atherosclerosis. J Vasc Surg. 2007. 46:1130–1137.19. Virani SS, Nambi V, Hoogeveen R, et al. Relationship between circulating levels of RANTES (regulated on activation, normal T-cell expressed, and secreted) and carotid plaque characteristics: the Atherosclerosis Risk in Communities (ARIC) Carotid MRI Study. Eur Heart J. 2011. 32:459–468.20. Degnan AJ, Young VE, Gillard JH. Advances in noninvasive imaging for evaluating clinical risk and guiding therapy in carotid atherosclerosis. Expert Rev Cardiovasc Ther. 2012. 10:37–53.21. Saam T, Yuan C, Chu B, et al. Predictors of carotid atherosclerotic plaque progression as measured by noninvasive magnetic resonance imaging. Atherosclerosis. 2007. 194:e34–e42.22. Lee JM, Robson MD, Yu LM, et al. Effects of high-dose modified-release nicotinic acid on atherosclerosis and vascular function: a randomized, placebo-controlled, magnetic resonance imaging study. J Am Coll Cardiol. 2009. 54:1787–1794.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- High-Resolusion Magnetic Resonance Imaging of Carotid Atherosclerotic Plaque
- Vessel Wall Imaging of the Intracranial and Cervical Carotid Arteries
- Carotid Ultrasound: Carotid Plaques and Clinical Significance
- Assessment of Carotid Diffusion-Weighted Imaging for Detection of Lipid-Rich Necrotic Core in Symptomatic Carotid Atheroma
- Noninvasive Imaging of Atherosclerotic Plaques Using MRI and CT
