Yonsei Med J.
2014 Nov;55(6):1526-1532. 10.3349/ymj.2014.55.6.1526.
Functional Class and Targeted Therapy Are Related to the Survival in Patients with Pulmonary Arterial Hypertension
- Affiliations
-
- 1Division of Cardiology, Heart Center, Gachon University Gil Hospital, Incheon, Korea. heart@gilhospital.com
- 2Gachon Cardiovascular Research Institute, Gachon University Gil Hospital, Incheon, Korea.
- 3Division of Pediatric Cardiology, Gachon University Gil Hospital, Incheon, Korea.
- 4Division of Rheumatology, Gachon University Gil Hospital, Incheon, Korea.
- 5Division of Pulmonology, Gachon University Gil Hospital, Incheon, Korea.
- KMID: 2070199
- DOI: http://doi.org/10.3349/ymj.2014.55.6.1526
Abstract
- PURPOSE
Pulmonary arterial hypertension (PAH) is an orphan disease showing poor prognosis. The purpose of study was to evaluate clinical factors influencing outcomes in PAH.
MATERIALS AND METHODS
Patients who were diagnosed with PAH at a single center were reviewed retrospectively. Forty patients (34.9+/-14.5 years, 80% of female) were enrolled.
RESULTS
Causes were congenital heart disease in 24 (60%), connective tissue disease in 8 (20%) and idiopathic PAH in 6 (15%). Sixteen patients (40%) were WHO functional class III or IV at the time of diagnosis. Twenty seven patients (67.5%) received molecular targeted therapy. During follow-up (53.6+/-45.5 months), 10 patients (25%) died and 1-, 2-, and 8 year survival rates were 91.3%, 78.7%, and 66.8%, respectively. As expected, median survival of patients with functional class I or II were significantly longer than patients with III or IV (p=0.041). Interestingly, patients with molecular targeted therapy showed longer survival than conventional therapy (p=0.021).
CONCLUSION
WHO functional class at the time of diagnosis was the strong predictor of survival, and molecular targeted therapy could significantly improve the survival. Therefore, early screening and intensive management would be crucial to improve the prognosis in the patient with PAH.
Keyword
MeSH Terms
-
Adult
Antihypertensive Agents/*therapeutic use
*Disease Management
Familial Primary Pulmonary Hypertension
Female
Heart Defects, Congenital/complications
Humans
Hypertension/complications
Hypertension, Pulmonary/*classification/*drug therapy/mortality
Kaplan-Meier Estimate
Male
Middle Aged
Molecular Targeted Therapy/*methods
Prognosis
Retrospective Studies
Survival Rate
Antihypertensive Agents
Figure
-
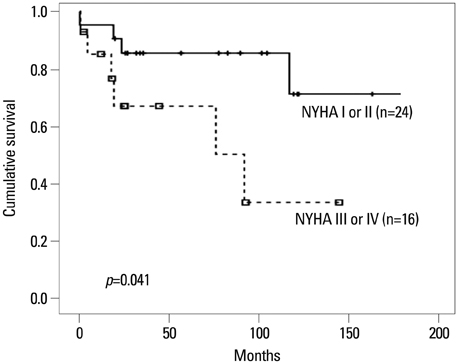
Fig. 1 Median overall survival time of patients by NYHA functional classification. Patients with NYHA class I or II at the time of diagnosis showed significantly better survival than those with more severe functional class.
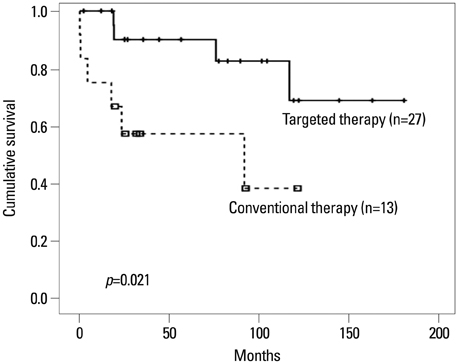
Fig. 2 Median overall survival time of patients according to the treatment. Patients with molecular targeted therapy showed significantly better survival than those with conventionally therapy only.
Cited by 1 articles
-
VEGF Promoter Polymorphism Confers an Increased Risk of Pulmonary Arterial Hypertension in a Chinese Population
Yufeng Zhuo, Qingchun Zeng, Peng Zhang, Guoyang Li, Qiang Xie, Ying Cheng
Yonsei Med J. 2017;58(2):305-311. doi: 10.3349/ymj.2017.58.2.305.
Reference
-
1. Farber HW, Loscalzo J. Pulmonary arterial hypertension. N Engl J Med. 2004; 351:1655–1665.
Article2. Badesch DB, Champion HC, Sanchez MA, Hoeper MM, Loyd JE, Manes A, et al. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol. 2009; 54:1 Suppl. S55–S66.
Article3. Chin KM, Rubin LJ. Pulmonary arterial hypertension. J Am Coll Cardiol. 2008; 51:1527–1538.
Article4. Weir EK, Rubin LJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. The acute administration of vasodilators in primary pulmonary hypertension. Experience from the National Institutes of Health Registry on Primary Pulmonary Hypertension. Am Rev Respir Dis. 1989; 140:1623–1630.
Article5. Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, Badesch DB, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med. 1996; 334:296–301.
Article6. Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009; 54:1 Suppl. S43–S54.
Article7. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation. 1978; 58:1072–1083.
Article8. Kircher BJ, Himelman RB, Schiller NB. Noninvasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am J Cardiol. 1990; 66:493–496.
Article9. Dabestani A, Mahan G, Gardin JM, Takenaka K, Burn C, Allfie A, et al. Evaluation of pulmonary artery pressure and resistance by pulsed Doppler echocardiography. Am J Cardiol. 1987; 59:662–668.
Article10. Opitz CF, Blindt R, Blumberg F, Borst MM, Bruch L, Leuchte H, et al. [Pulmonary hypertension: hemodynamic evaluation: hemodynamic evaluation - recommendations of the Cologne Consensus Conference 2010]. Dtsch Med Wochenschr. 2010; 135:Suppl 3. S78–S86.11. Jing ZC, Jiang X, Han ZY, Xu XQ, Wang Y, Wu Y, et al. Iloprost for pulmonary vasodilator testing in idiopathic pulmonary arterial hypertension. Eur Respir J. 2009; 33:1354–1360.
Article12. D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991; 115:343–349.13. Olivari MT. Primary pulmonary hypertension. Am J Med Sci. 1991; 302:185–198.14. Sitbon O, Humbert M, Nunes H, Parent F, Garcia G, Hervé P, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol. 2002; 40:780–788.
Article15. McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation. 2002; 106:1477–1482.16. Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med. 2004; 351:1425–1436.
Article17. Barst RJ, Rubin LJ, McGoon MD, Caldwell EJ, Long WA, Levy PS. Survival in primary pulmonary hypertension with long-term continuous intravenous prostacyclin. Ann Intern Med. 1994; 121:409–415.
Article18. Simonneau G, Barst RJ, Galie N, Naeije R, Rich S, Bourge RC, et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med. 2002; 165:800–804.
Article19. Olschewski H, Simonneau G, Galiè N, Higenbottam T, Naeije R, Rubin LJ, et al. Inhaled iloprost for severe pulmonary hypertension. N Engl J Med. 2002; 347:322–329.
Article20. McLaughlin VV, McGoon MD. Pulmonary arterial hypertension. Circulation. 2006; 114:1417–1431.
Article21. Galiè N, Torbicki A, Barst R, Dartevelle P, Haworth S, Higenbottam T, et al. Guidelines on diagnosis and treatment of pulmonary arterial hypertension. The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hypertension of the European Society of Cardiology. Eur Heart J. 2004; 25:2243–2278.22. Sohn DW, Kim HK, Kim MA, Song YW, Noh CI, Kim DK, et al. Beneficial and adverse effects of bosentan treatment in Korean patients with pulmonary artery hypertension. Korean Circ J. 2009; 39:105–110.
Article23. Chung WJ. Treatment of pulmonary hypertension. Korean J Med. 2010; 78:28–35.24. Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J. 2009; 30:2493–2537.25. Task Force for Diagnosis and Treatment of Pulmonary Hypertension of European Society of Cardiology (ESC). European Respiratory Society (ERS). International Society of Heart and Lung Transplantation (ISHLT). Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009; 34:1219–1263.
Article26. Kemp K, Savale L, O'Callaghan DS, Jaïs X, Montani D, Humbert M, et al. Usefulness of first-line combination therapy with epoprostenol and bosentan in pulmonary arterial hypertension: an observational study. J Heart Lung Transplant. 2012; 31:150–158.
Article27. Fuster V, Steele PM, Edwards WD, Gersh BJ, McGoon MD, Frye RL. Primary pulmonary hypertension: natural history and the importance of thrombosis. Circulation. 1984; 70:580–587.
Article28. Lee WS, Kim KH, Jeong DH, Lee KH, Hong SN, Park HW, et al. Clinical characteristics and prognostic factors of patients with severe pulmonary hypertension. Korean Circ J. 2007; 37:265–270.
Article29. Rich S, Dantzker DR, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med. 1987; 107:216–223.30. Lee WD, Kim DS, Lee JH, Cho KI, Cho KH, Kim DK, et al. A clinical review of primary pulmonary hypertension. Korean Circ J. 2003; 33:507–512.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis and treatment of idiopathic pulmonary arterial hypertension
- Pulmonary Arterial Hypertension is Normalized Following Six Years of Inhaled Iloprost Treatment in a Patient with Systemic Sclerosis
- Updated clinical classification of pulmonary hypertension
- Pulmonary Arterial Hypertension
- Overview and Evaluation of Pulmonary Hypertension
