Mini-Gastric Bypass to Control Morbid Obesity and Diabetes Mellitus: What Radiologists Need to Know
- Affiliations
-
- 1Department of Radiology, Chung-Ang University Hospital, Seoul 156-755, Korea.
- 2Department of Radiology, Soonchunhyang University Seoul Hospital, Seoul 140-743, Korea. hongses@schmc.ac.kr
- 3Department of Surgery, Soonchunhyang University Seoul Hospital, Seoul 140-743, Korea.
- KMID: 2070176
- DOI: http://doi.org/10.3348/kjr.2015.16.2.325
Abstract
- Laparoscopic mini-gastric bypass surgery is a safe and simple surgical intervention for treating morbid obesity and diabetes mellitus and is now being performed more frequently. Radiologists must be critical in their postoperative evaluation of these patients. In this pictorial review, we explain and illustrate the surgical technique, normal postoperative anatomy, and associated complications as seen on imaging examinations, including fluoroscopy and computed tomography.
MeSH Terms
Figure
-
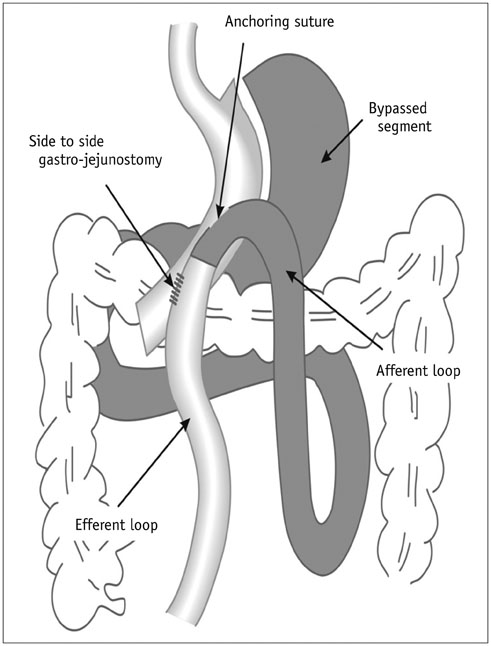
Fig. 1 Illustration of laparoscopic mini-gastric bypass. Mini-gastric tube is mounted parallel from angle of His to 2 cm proximal to pylorus along lesser curvature. Anchoring suture is used for acute angulation, and antecolic side-to-side gastro-jejunostomy is formed 200 cm distal to Treitz ligament. Bypassed segment is denoted by gray zone.

Fig. 2 Normal upper gastrointestinal series on postoperative day 1. A. No obvious contrast leakage or luminal narrowing is seen at side-to-side gastro-jejunostomy site (arrows). Afferent loop is not typically detected, and faint staple lines (arrowheads) are detected along gastric curvature. B. Image in another patient shows afferent loop (curved arrow) partially and multiple clips (arrows) with faint staple lines to prevent bleeding. E = efferent loop
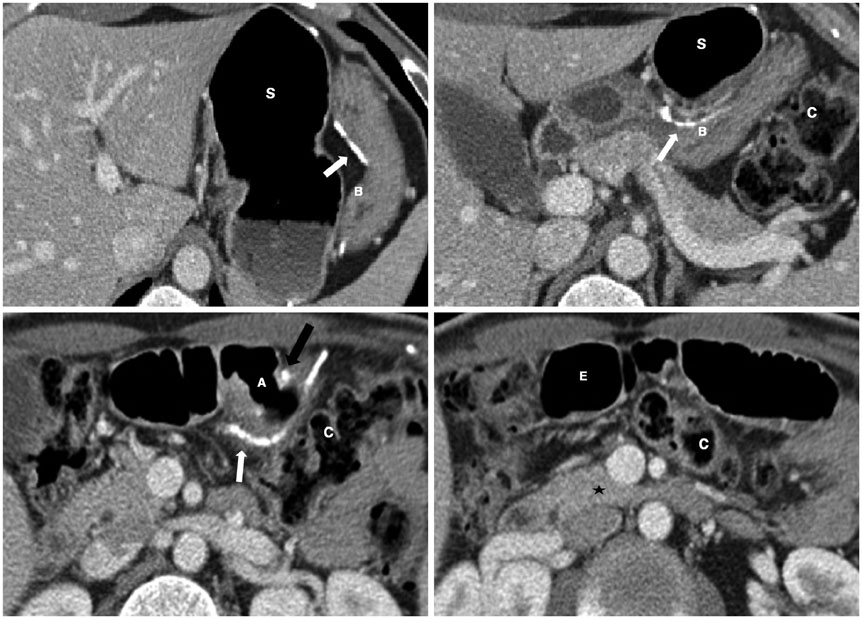
Fig. 3 Computed tomography (CT) scans after mini-gastric bypass surgery. Cranial to caudal CT scans reveal remnant stomach (S) and bypassed segment (B). Gastro-jejunostomy (A) and distal loop (E) are anterior to transverse colon (C). Third duodenum (*) is marker to identify afferent loop. Staples for gastric separation are indicated by white arrows, and side-to-side gastro-jejunostomy is indicated by black arrow.
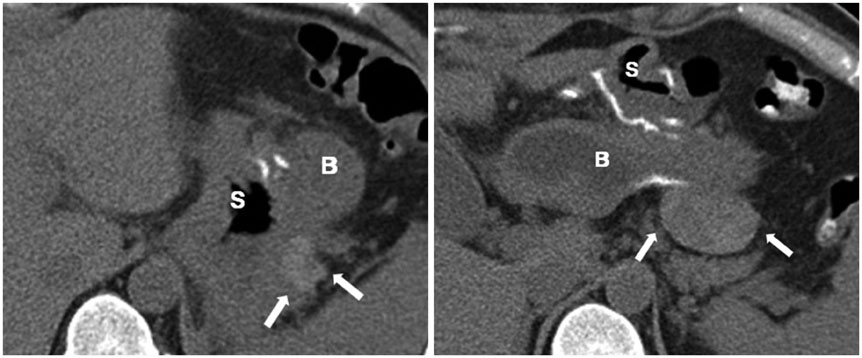
Fig. 4 Formation of hematoma in 31-year-old woman with decreased hemoglobin level. Pre-contrast computed tomography scans reveal high density fluid (arrows) (mean, 58 Hounsfield units) around remnant stomach (S) adjacent to staples without extravasation. Bleeding was spontaneously controlled. B = bypassed segment
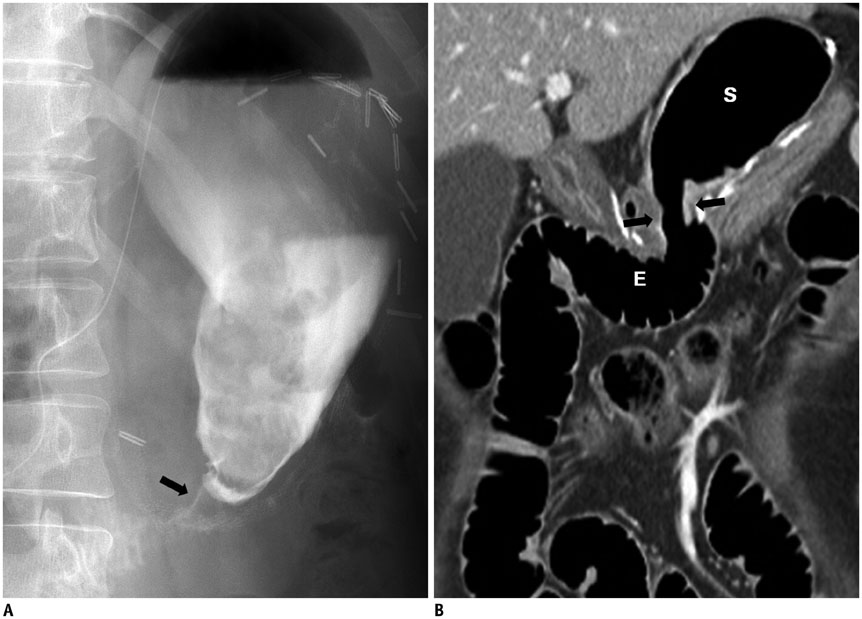
Fig. 5 Anastomotic narrowing in 37-year-old man. A. Remnant stomach was distended on upper gastrointestinal series due to passage disturbance on postoperative day 1. String-like narrowing at gastro-jejunostomy (arrow) was probably caused by postoperative edema. Follow-up X-ray 4 hours later shows unimpeded passage of contrast agent into large intestine (not shown). B. Follow-up coronal computed tomography scan after 3 months reveals improvement in narrowing of gastro-jejunostomy (arrows) and no evidence of complications. E = efferent loop, S = remnant stomach
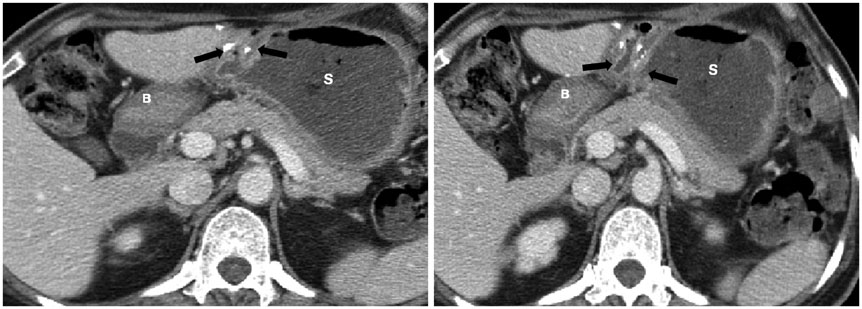
Fig. 6 Anastomotic stenosis in 49-year-old woman with postprandial abdominal pain 6 months postoperatively. Axial computed tomography scans reveal distension of remnant stomach (S) and narrowing of gastro-jejunostomy (arrows), suggesting anastomotic stenosis. B = bypassed segment

Fig. 7 Formation of abscess in 53-year-old woman with fever on postoperative day 15. Axial (A) and coronal (B) computed tomography scans show rim enhancement and loculated fluid (*) around pancreas with adjacent fat stranding. Percutaneous drainage with catheter produced odorous abscess. B = bypassed segment, S = remnant stomach
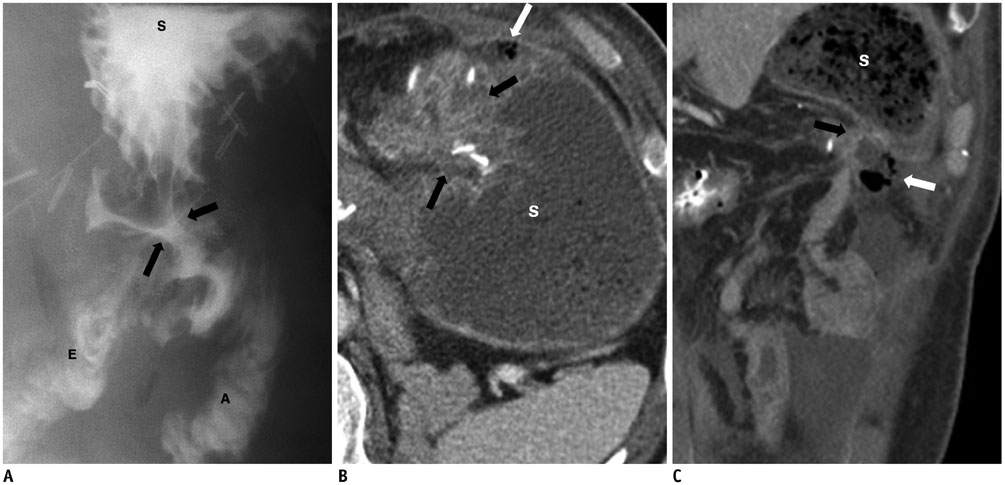
Fig. 8 Anastomotic leak in 46-year-old man with abdominal pain on postoperative day 7. A. Upper gastrointestinal series on postoperative day 1 shows edematous changes in gastro-jejunostomy (black arrows) without obvious contrast agent leak or passage disturbance. B, C. Axial (B) and coronal (C) computed tomography scans obtained on postoperative day 7 reveal air containing fluid (white arrows) adjacent to anastomosed site (black arrows) and ascites around lesion and left paracolic gutter. A = afferent loop, E = efferent loop, S = stomach
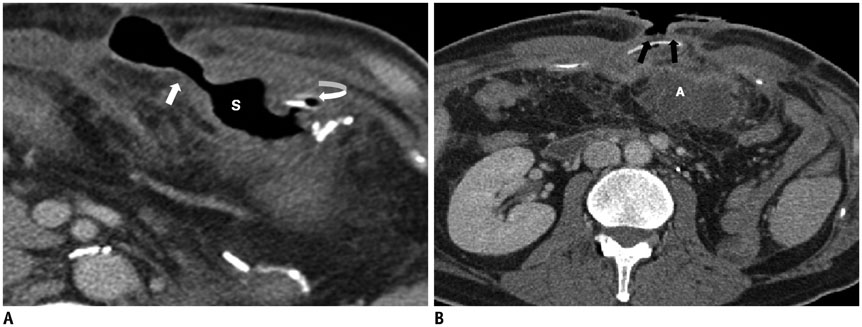
Fig. 9 Wound complications in 46-year-old man who underwent additional Roux-en-Y gastric bypass jejunostomy to treat leak. A. Computed tomography (CT) scan obtained on postoperative day 37 reveals direct connection (arrow) between remnant stomach and subcutaneous tissue, presenting as gastro-cutaneous fistula. Curved arrow = gastrojejunostomy. B. CT scan obtained on postoperative day 97 reveals wound dehiscence (arrows) and skin thickening. Intra-abdominal abscess (A) and mesenteric fat infiltration with peritoneal thickening are seen with secondary edematous changes in bowel loops. S = remnant stomach

Fig. 10 Marginal ulcer perforation in 65-year-old woman with sudden abdominal pain 1 year after surgery. Axial computed tomography scans reveal focal wall defect (arrows) in efferent loop (E) just below gastro-jejunostomy (A) with pneumoperitoneum (*), associated with edematous wall thickening in remnant stomach (S) as well as efferent loop with mesenteric haziness. B = bypassed segment

Fig. 11 Acute cholecystitis in 62-year-old woman with upper abdominal pain 1 year after surgery. A. Abdominal ultrasonography reveals sandy stones and sludge (curved arrow) in distended gall bladder (GB) with wall thickening. B. Computed tomography scan on same day shows distended GB with wall thickening and hyperemia (arrows) of adjacent liver.
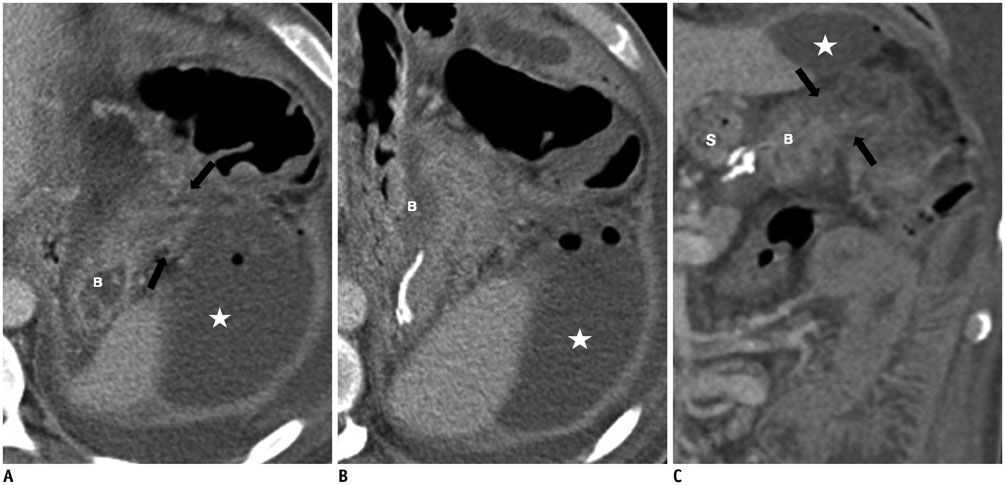
Fig. 12 Spontaneous perforation in bypassed segment of 39-year-old man with generalized abdominal pain 8 months after surgery. Axial (A, B) and coronal (C) computed tomography scans show focal edematous wall thickening and suspicious wall defect (arrows) in upper greater curvature of bypassed gastric segment (B), which was away from staples, with abscess forming (*) around lesion, presumably peptic ulcer with perforation that was surgically proven. S = remnant stomach
Reference
-
1. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991; 115:956–961.2. Pories WJ, Swanson MS, MacDonald KG, Long SB, Morris PG, Brown BM, et al. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg. 1995; 222:339–350. discussion 350-352.3. O'Brien PE, Dixon JB, Laurie C, Skinner S, Proietto J, McNeil J, et al. Treatment of mild to moderate obesity with laparoscopic adjustable gastric banding or an intensive medical program: a randomized trial. Ann Intern Med. 2006; 144:625–633.4. Adams TD, Gress RE, Smith SC, Halverson RC, Simper SC, Rosamond WD, et al. Long-term mortality after gastric bypass surgery. N Engl J Med. 2007; 357:753–761.5. Schauer PR, Burguera B, Ikramuddin S, Cottam D, Gourash W, Hamad G, et al. Effect of laparoscopic Roux-en Y gastric bypass on type 2 diabetes mellitus. Ann Surg. 2003; 238:467–484. discussion 484-485.6. Lee WJ, Wang W, Lee YC, Huang MT, Ser KH, Chen JC. Effect of laparoscopic mini-gastric bypass for type 2 diabetes mellitus: comparison of BMI>35 and <35 kg/m2. J Gastrointest Surg. 2008; 12:945–952.7. Brethauer SA, Aminian A, Romero-Talamás H, Batayyah E, Mackey J, Kennedy L, et al. Can diabetes be surgically cured? Long-term metabolic effects of bariatric surgery in obese patients with type 2 diabetes mellitus. Ann Surg. 2013; 258:628–636. discussion 636-637.8. Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Brethauer SA, Navaneethan SD, et al. Bariatric surgery versus intensive medical therapy for diabetes--3-year outcomes. N Engl J Med. 2014; 370:2002–2013.9. Lee WJ, Yu PJ, Wang W, Chen TC, Wei PL, Huang MT. Laparoscopic Roux-en-Y versus mini-gastric bypass for the treatment of morbid obesity: a prospective randomized controlled clinical trial. Ann Surg. 2005; 242:20–28.10. Lee WJ, Ser KH, Lee YC, Tsou JJ, Chen SC, Chen JC. Laparoscopic Roux-en-Y vs. mini-gastric bypass for the treatment of morbid obesity: a 10-year experience. Obes Surg. 2012; 22:1827–1834.11. Musella M, Susa A, Greco F, De Luca M, Manno E, Di Stefano C, et al. The laparoscopic mini-gastric bypass: the Italian experience: outcomes from 974 consecutive cases in a multicenter review. Surg Endosc. 2014; 28:156–163.12. Rutledge R, Walsh TR. Continued excellent results with the mini-gastric bypass: six-year study in 2,410 patients. Obes Surg. 2005; 15:1304–1308.13. Greenfield LJ. Complications of gastric surgery. In : Greenfield LJ, editor. Complications in surgery and trauma. Philadelphia: Lippincott;1990. p. 457–467.14. Yu J, Turner MA, Cho SR, Fulcher AS, DeMaria EJ, Kellum JM, et al. Normal anatomy and complications after gastric bypass surgery: helical CT findings. Radiology. 2004; 231:753–760.15. Byrne TK. Complications of surgery for obesity. Surg Clin North Am. 2001; 81:1181–1193. vii-viii.16. Akkary E, Duffy A, Bell R. Deciphering the sleeve: technique, indications, efficacy, and safety of sleeve gastrectomy. Obes Surg. 2008; 18:1323–1329.17. Koehler RE, Halverson JD. Radiographic abnormalities after gastric bypass. AJR Am J Roentgenol. 1982; 138:267–270.18. Blachar A, Federle MP. Gastrointestinal complications of laparoscopic roux-en-Y gastric bypass surgery in patients who are morbidly obese: findings on radiography and CT. AJR Am J Roentgenol. 2002; 179:1437–1442.19. Podnos YD, Jimenez JC, Wilson SE, Stevens CM, Nguyen NT. Complications after laparoscopic gastric bypass: a review of 3464 cases. Arch Surg. 2003; 138:957–961.20. Carbajo M, García-Caballero M, Toledano M, Osorio D, García-Lanza C, Carmona JA. One-anastomosis gastric bypass by laparoscopy: results of the first 209 patients. Obes Surg. 2005; 15:398–404.21. Noun R, Skaff J, Riachi E, Daher R, Antoun NA, Nasr M. One thousand consecutive mini-gastric bypass: short- and long-term outcome. Obes Surg. 2012; 22:697–703.22. Csendes A, Burdiles P, Burgos AM, Maluenda F, Diaz JC. Conservative management of anastomotic leaks after 557 open gastric bypasses. Obes Surg. 2005; 15:1252–1256.23. Jordan JH, Hocking MP, Rout WR, Woodward ER. Marginal ulcer following gastric bypass for morbid obesity. Am Surg. 1991; 57:286–288.24. Rasmussen JJ, Fuller W, Ali MR. Marginal ulceration after laparoscopic gastric bypass: an analysis of predisposing factors in 260 patients. Surg Endosc. 2007; 21:1090–1094.25. Wang W, Wei PL, Lee YC, Huang MT, Chiu CC, Lee WJ. Short-term results of laparoscopic mini-gastric bypass. Obes Surg. 2005; 15:648–654.26. Papavramidis S, Deligianidis N, Papavramidis T, Sapalidis K, Katsamakas M, Gamvros O. Laparoscopic cholecystectomy after bariatric surgery. Surg Endosc. 2003; 17:1061–1064.27. Fidler J, Paulson EK, Layfield L. CT evaluation of acute cholecystitis: findings and usefulness in diagnosis. AJR Am J Roentgenol. 1996; 166:1085–1088.28. Macgregor AM, Pickens NE, Thoburn EK. Perforated peptic ulcer following gastric bypass for obesity. Am Surg. 1999; 65:222–225.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Morbid Obesity
- Metabolic Surgery and Diabetes Mellitus: Its Effects and Side Effects
- Mechanism of Metabolic Improvement After Bariatric Surgery
- Effects of Bariatric Surgery in Type 2 Diabetes Mellitus
- A Gut Feeling to Cure Diabetes: Potential Mechanisms of Diabetes Remission after Bariatric Surgery
