Limited Unilateral Decompression and Pedicle Screw Fixation with Fusion for Lumbar Spinal Stenosis with Unilateral Radiculopathy: A Retrospective Analysis of 25 Cases
- Affiliations
-
- 1Department of Orthopedic Surgery, Peking University Third Hospital, Beijing, China. liuxiaoguangpku@163.com
- 2Department of Orthopedic Surgery, Huizhou First Hospital, Guangdong, China.
- 3Department of Surgery, Beijing North Hospital of Ordnance Industry, Beijing, China.
- 4Department of Orthopedic Surgery, General Hospital of Huabei Oil Field Company, Hebei, China.
- KMID: 2067107
- DOI: http://doi.org/10.3340/jkns.2015.58.1.65
Abstract
OBJECTIVE
Lumbar spinal stenosis is conventionally treated with surgical decompression. However, bilateral decompression and laminectomy is more invasive and may not be necessary for lumbar stenosis patients with unilateral radiculopathy. We aimed to report the outcomes of unilateral laminectomy and bilateral pedicle screw fixation with fusion for patients with lumbar spinal stenosis and unilateral radiculopathy.
METHODS
Patients with lumbar spinal stenosis with unilateral lower extremity radiculopathy who received limited unilateral decompression and bilateral pedicle screw fixation were included and evaluated using visual analog scale (VAS) pain and the Oswestry Disability Index (ODI) scores preoperatively and at follow-up visits. Ligamentum flavum thickness of the involved segments was measured on axial magnetic resonance images.
RESULTS
Twenty-five patients were included. The mean preoperative VAS score was 6.6+/-1.6 and 4.6+/-3.1 for leg and back pain, respectively. Ligamentum flavum thickness was comparable between the symptomatic and asymptomatic side (p=0.554). The mean follow-up duration was 29.2 months. The pain in the symptomatic side lower extremity (VAS score, 1.32+/-1.2) and the back (VAS score, 1.75+/-1.73) significantly improved (p=0.000 vs. baseline for both). The ODI improved significantly postoperatively (6.60+/-6.5; p=0.000 vs. baseline). Significant improvement in VAS pain and ODI scores were observed in patients receiving single or multi-segment decompression fusion with fixation (p<0.01).
CONCLUSION
Limited laminectomy and unilateral spinal decompression followed by bilateral pedicle screw fixation with fusion achieves satisfactory outcomes in patients with spinal stenosis and unilateral radiculopathy. This procedure is less damaging to structures that are important for maintaining posterior stability of the spine.
Keyword
MeSH Terms
Figure
-
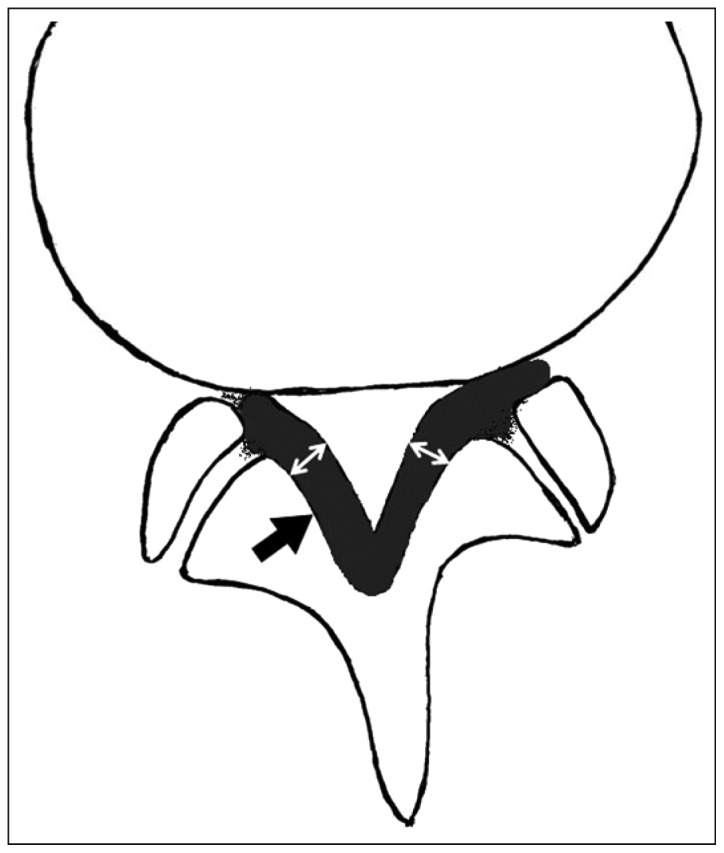
Fig. 1 Schematic drawing of ligamentum flavum thickness measurement. Solid arrow indicates the ligamentum flavum and double white arrow indicates the thickest portion of the ligamentum flavum where measurement was made.
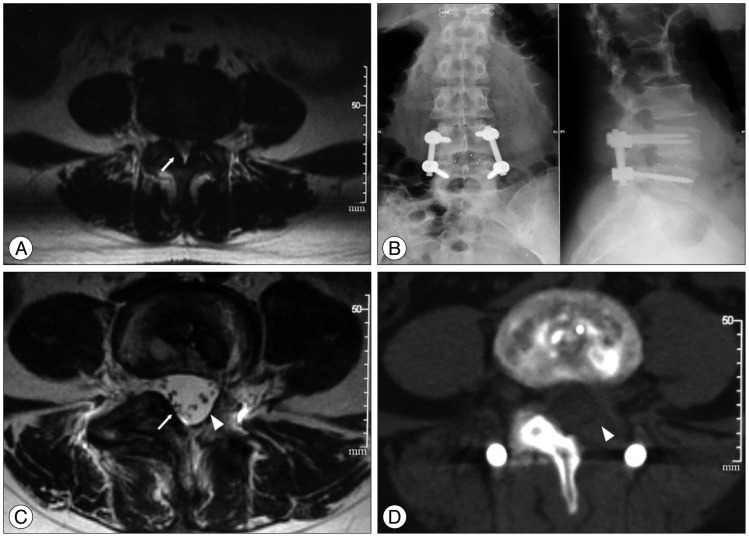
Fig. 2 A 42-year-old female with spinal stenosis accompanied by unilateral radiculopathy of the left lower extremity for 1 year. A : Preoperative MRI revealed thickening of the ligamentum flavum (by white arrow). The symptomatic (L)/asymptomatic (R) ratio of bilateral ligamentum thickness at L4/5=1.24. B : Bilateral L4/5 pedicle screw fixation, left decompression TLIF were performed. C : Postoperative MRI. The white triangle points to L4/L5 with left hemilaminectomy and excision of the ligamentum flavum. White arrow shows the intact right side. D : Postoperative CT showed left hemilaminectomy (arrow).
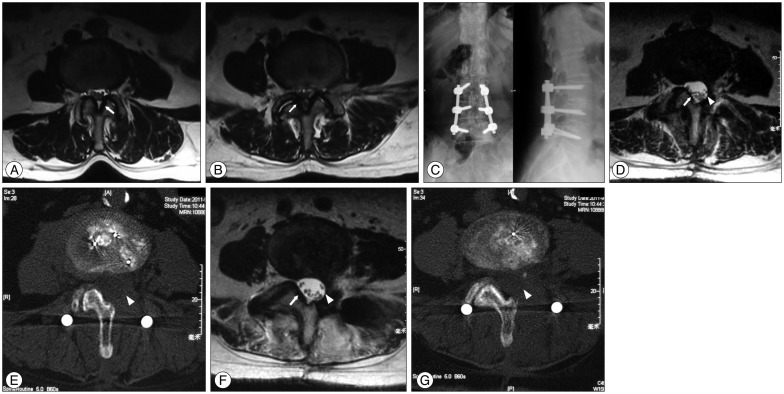
Fig. 3 A 61-year-old female with intermittent back pain for more than 10 years, accompanied by posterolateral radiating pain of the left lower leg with intermittent claudication for more than 2 years. A : Preoperative MRI revealed bilateral L3-4 ligamentum flavum thickening. White arrow indicates thickness on the left side was greater than the right side. B : Preoperative MRI revealed bilateral L4-5 ligamentum flavum thickening. White arrow indicates thickness on the right side was greater than on the left side. C : Bilateral pedicle screw fixation was performed at L3 to L5, and the right laminae and facet joints at L3 to L5 received morselized bone graft. L3-5 left lamina and ligamentum flavum were partially excised, and transforaminal lumbar interbody fusion was performed. D : Postoperative MRI. The white triangle points to L4/5 with left hemilaminectomy and excision of the ligamentum flavum. White arrow shows the normal right side. E : Postoperative MRI. The white triangle points to L3/4 with left hemilaminectomy and excision of the ligamentum flavum. F : Postoperative MRI of L4/5 intervertebral space. The pointed white triangle indicates the left (symptomatic) vertebral plate and the excised ligamentum flavum. Dural sac decompression and bulging are satisfactory. White arrow indicates the right (asymptomatic) vertebral plate and ligamentum flavum. G : Postoperative CT scan of L4/5 intervertebral space. The pointed white triangle indicates left (symptomatic) vertebral plate and the excised ligamentum flavum. Dural sac decompression and bulging are satisfactory.
Reference
-
1. Adams MA, Hutton WC, Stott JR. The resistance to flexion of the lumbar intervertebral joint. Spine (Phila Pa 1976). 1980; 5:245–253. PMID: 7394664.
Article2. Altinkaya N, Yildirim T, Demir S, Alkan O, Sarica FB. Factors associated with the thickness of the ligamentum flavum : is ligamentum flavum thickening due to hypertrophy or buckling? Spine (Phila Pa 1976). 2011; 36:E1093–E1097. PMID: 21343862.3. Amundsen T, Weber H, Lilleås F, Nordal HJ, Abdelnoor M, Magnaes B. Lumbar spinal stenosis. Clinical and radiologic features. Spine (Phila Pa 1976). 1995; 20:1178–1186. PMID: 7638662.4. Capogna G, Celleno D, Simonetti C, Lupoi D. Anatomy of the lumbar epidural region using magnetic resonance imaging : a study of dimensions and a comparison of two postures. Int J Obstet Anesth. 1997; 6:97–100. PMID: 15321289.
Article5. Haig AJ, Adewole A, Yamakawa KS, Kelemen B, Aagesen AL. The ligamentum flavum at L4-5 : relationship with anthropomorphic factors and clinical findings in older persons with and without spinal disorders. PM R. 2012; 4:23–29. PMID: 22093441.
Article6. Hindle RJ, Pearcy MJ, Cross A. Mechanical function of the human lumbar interspinous and supraspinous ligaments. J Biomed Eng. 1990; 12:340–344. PMID: 2395361.
Article7. Hong SW, Choi KY, Ahn Y, Baek OK, Wang JC, Lee SH, et al. A comparison of unilateral and bilateral laminotomies for decompression of L4-L5 spinal stenosis. Spine (Phila Pa 1976). 2011; 36:E172–E178. PMID: 21192307.
Article8. Kasai Y, Inaba T, Kato T, Matsumura Y, Akeda K, Uchida A. Biomechanical study of the lumbar spine using a unilateral pedicle screw fixation system. J Clin Neurosci. 2010; 17:364–367. PMID: 20071182.
Article9. Kreiner DS, Shaffer WO, Baisden JL, Gilbert TJ, Summers JT, Toton JF, et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update). Spine J. 2013; 13:734–743. PMID: 23830297.
Article10. Lohman CM, Tallroth K, Kettunen JA, Lindgren KA. Comparison of radiologic signs and clinical symptoms of spinal stenosis. Spine (Phila Pa 1976). 2006; 31:1834–1840. PMID: 16845360.
Article11. Louis R, Nazarian S. Lumbar stenosis surgery : the experience of the orthopaedic surgeon. Chir Organi Mov. 1992; 77:23–29. PMID: 1587157.12. Olszewski AD, Yaszemski MJ, White AA 3rd. The anatomy of the human lumbar ligamentum flavum. New observations and their surgical importance. Spine (Phila Pa 1976). 1996; 21:2307–2312. PMID: 8915063.13. Park JB, Chang H, Lee JK. Quantitative analysis of transforming growth factor-beta 1 in ligamentum flavum of lumbar spinal stenosis and disc herniation. Spine (Phila Pa 1976). 2001; 26:E492–E495. PMID: 11679833.
Article14. Periasamy K, Shah K, Wheelwright EF. Posterior lumbar interbody fusion using cages, combined with instrumented posterolateral fusion : a study of 75 cases. Acta Orthop Belg. 2008; 74:240–248. PMID: 18564483.15. Safak AA, Is M, Sevinc O, Barut C, Eryoruk N, Erdogmus B, et al. The thickness of the ligamentum flavum in relation to age and gender. Clin Anat. 2010; 23:79–83. PMID: 19941359.
Article16. Sengupta DK, Herkowitz HN. Lumbar spinal stenosis. Treatment strategies and indications for surgery. Orthop Clin North Am. 2003; 34:281–295. PMID: 12914268.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unilateral versus Bilateral Pedide Scrwe Fixation in Lumbar Spinal Fusion
- Unilateral Pedicle Screw Fixation in Degenerative Lumbar Spinal Stenosis
- Mini-invasive unilateral transforaminal lumbar interbody fusion and pedicle screw fixation
- Cotrel - Dubousset Pedicle Screw Fixation After Posterior Decompression of Lumbar Spinal Stenosis
- Minimally Invasive Lumbar Decompression, Interbody Fusion, and Pedicle Screw Fixation: Preliminary Report
