Short Segment Screw Fixation without Fusion for Unstable Thoracolumbar and Lumbar Burst Fracture : A Prospective Study on Selective Consecutive Patients
- Affiliations
-
- 1Department of Neurosurgery, School of Medicine, Chosun University, Gwangju, Korea. chosunns@hanmail.net
- 2Department of Neurosurgery, Heori Sarang Hospital, Daejeon, Korea.
- 3Gyeryoung Orthopedic Surgery Clinic, Daejeon, Korea.
- KMID: 2066911
- DOI: http://doi.org/10.3340/jkns.2012.51.4.203
Abstract
OBJECTIVE
The purpose of this prospective study was to evaluate the efficacy and safety of screw fixation without bone fusion for unstable thoracolumbar and lumbar burst fracture.
METHODS
Nine patients younger than 40 years underwent screw fixation without bone fusion, following postural reduction using a soft roll at the involved vertebra, in cases of burst fracture. Their motor power was intact in spite of severe canal compromise. The surgical procedure included postural reduction for 3 days and screw fixations at one level above, one level below and at the fractured level itself. The patients underwent removal of implants 12 months after the initial operation, due to possibility of implant failure. Imaging and clinical findings, including canal encroachment, vertebral height, clinical outcome, and complications were analyzed.
RESULTS
Prior to surgery, the mean pain score (visual analogue scale) was 8.2, which decreased to 2.2 at 12 months after screw fixation. None of the patients complained of worsening of pain during 6 months after implant removal. All patients were graded as having excellent or good outcomes at 6 months after implant removal. The proportion of canal compromise at the fractured level improved from 55% to 35% at 12 months after surgery. The mean preoperative vertebral height loss was 45.3%, which improved to 20.6% at 6 months after implant removal. There were no neurological deficits related to neural injury. The improved vertebral height and canal compromise were maintained at 6 months after implant removal.
CONCLUSION
Short segment pedicle screw fixation, including fractured level itself, without bone fusion following postural reduction can be an effective and safe operative technique in the management of selected young patients suffering from unstable burst fracture.
Keyword
Figure
-

Fig. 1 Fraction of canal compromise. *p=0.008 for preoperative versus 12 months after screw fixation. **p=0.008 for preoperative versus 6 months implant removal.
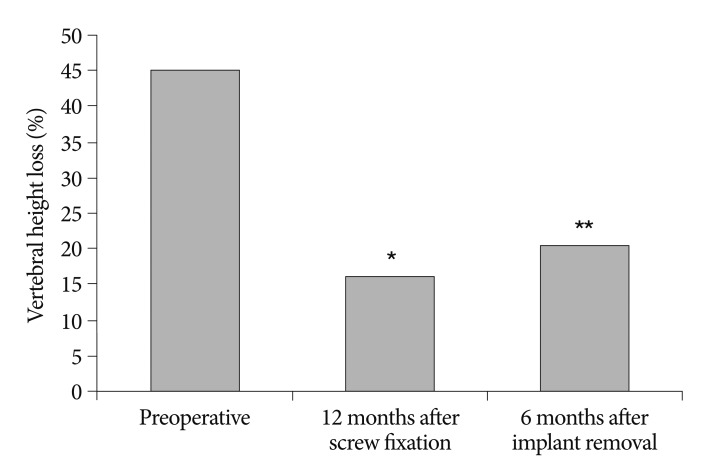
Fig. 2 Restoration of vertebral height. *p=0.001 for preoperative versus 12 months after screw fixation. **p=0.005 for preoperative versus 6 months implant removal.
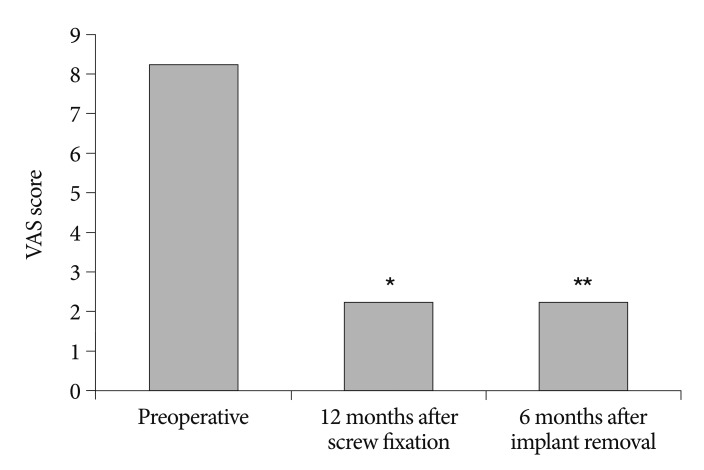
Fig. 3 Improvement of pain score. *p=0.001 for preoperative versus 12 months after screw fixation. **p=0.002 for preoperative versus 6 months implant removal.
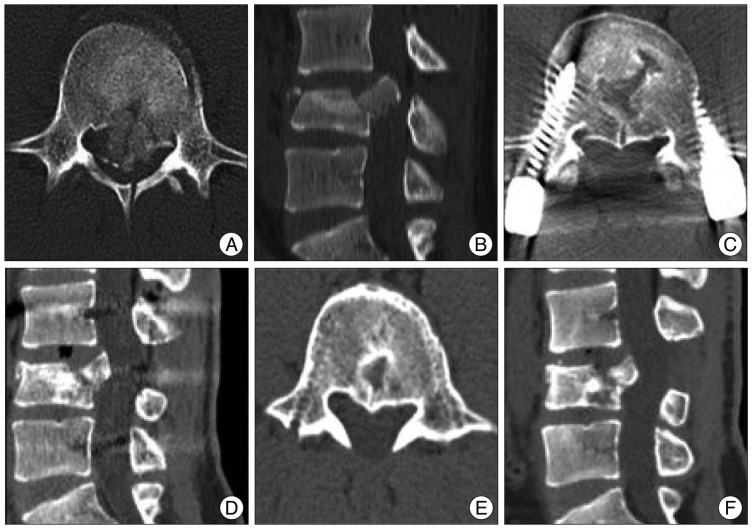
Fig. 4 A neurologically intact 16-year-old male patient fell down and sustained L4 bursting fracture. A and B : Preoperative computed tomography scans show severe canal compromise (about 80%) and spinous process fracture. C and D : Computed tomographic scans at 12 months follow-up, just before implant removal demonstrate bone healing and canal remodeling with improved canal compromise. E and F : Computed tomographic scans at 6 months after implant removal reveal well-maintained improved canal compromise.

Fig. 5 A neurologically intact 19-year-old female patient fell down and sustained L2 bursting fracture. A and B : Preoperative computed tomography scans show severe canal compromise (about 60%) and spinous process fracture. C and D : Computed tomographic scans at 12 months follow-up, just before implant removal demonstrate bone healing and canal remodeling with improved canal compromise. E and F : Computed tomographic scans at 6 months after implant removal reveal well-maintained improved canal compromise.
Cited by 2 articles
-
Short Segment Fixation for Thoracolumbar Burst Fracture Accompanying Osteopenia : A Comparative Study
Hyeun Sung Kim, Seok Won Kim, Chang Il Ju, Sung Myung Lee, Ho Shin
J Korean Neurosurg Soc. 2013;53(1):26-30. doi: 10.3340/jkns.2013.53.1.26.Implant Removal after Percutaneous Short Segment Fixation for Thoracolumbar Burst Fracture : Does It Preserve Motion?
Hyeun Sung Kim, Seok Won Kim, Chang Il Ju, Hui Sun Wang, Sung Myung Lee, Dong Min Kim
J Korean Neurosurg Soc. 2014;55(2):73-77. doi: 10.3340/jkns.2014.55.2.73.
Reference
-
1. Carl AL, Tromanhauser SG, Roger DJ. Pedicle screw instrumentation for thoracolumbar burst fractures and fracture-dislocations. Spine (Phila Pa 1976). 1992; 17:S317–S324. PMID: 1523519.
Article2. Cho WS, Chung CK, Jahng TA, Kim HJ. Post-laminectomy kyphosis in patients with cervical ossification of the posterior longitudinal ligament : does it cause neurological deterioration? J Korean Neurosurg Soc. 2008; 43:259–264. PMID: 19096629.
Article3. de Klerk LW, Fontijne WP, Stijnen T, Braakman R, Tanghe HL, van Linge B. Spontaneous remodeling of the spinal canal after conservative management of thoracolumbar burst fractures. Spine (Phila Pa 1976). 1998; 23:1057–1060. PMID: 9589546.
Article4. Jang KS, Ju CI, Kim SW, Lee SM. Screw fixation without fusion for low lumbar burst fracture : a severe canal compromise but neurologically intact case. J Korean Neurosurg Soc. 2011; 49:128–130. PMID: 21519504.
Article5. Kostuik JP. Anterior fixation for burst fractures of the thoracic and lumbar spine with or without neurological involvement. Spine (Phila Pa 1976). 1988; 13:286–293. PMID: 2455351.
Article6. Lin HJ, Wang ST, Liu CL. Reduction fixation system in treating burst fractures of thoracolumbar spine. J Spine Surg ROC. 1996; 2:102–111.7. Liu CL, Dai LG, Wang ST. Surgical treatment of thoracic spine burst fractures. J Spine Surg ROC. 1996; 2:92–101.8. Liu CL, Wang ST, Lin HJ, Kao HC, Yu WK, Lo WH. Roy-Camille plating system in treating burst fractures of thoracolumbar spine. J Orthop Surg Roc. 1996; 13:309–316.9. Mueller LA, Mueller LP, Schmidt R, Forst R, Rudig L. The phenomenon and efficiency of ligamentotaxis after dorsal stabilization of thoracolumbar burst fractures. Arch Orthop Trauma Surg. 2006; 126:364–368. PMID: 16721620.
Article10. Mumford J, Weinstein JN, Spratt KF, Goel VK. Thoracolumbar burst fractures. The clinical efficacy and outcome of nonoperative management. Spine (Phila Pa 1976). 1993; 18:955–970. PMID: 8367783.11. Sanderson PL, Fraser RD, Hall DJ, Cain CM, Osti OL, Potter GR. Short segment fixation of thoracolumbar burst fractures without fusion. Eur Spine J. 1999; 8:495–500. PMID: 10664310.
Article12. Scapinelli R, Candiotto S. Spontaneous remodeling of the spinal canal after burst fractures of the low thoracic and lumbar region. J Spinal Disord. 1995; 8:486–493. PMID: 8605423.
Article13. Sjostrom L, Karlstrom G, Pech P, Rauschning W. Indirect spinal canal decompression in burst fractures treated with pedicle screw instrumentation. Spine (Phila Pa 1976). 1996; 21:113–123. PMID: 9122751.
Article14. Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999; 24:412–415. PMID: 10065527.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Short- and Long-segment Pedicle Screw Fixation with Anterior Interbody Fusion with Short Bone Graft in Denis type B Burst Fractures
- Short Segment Fixation for Thoracolumbar Burst Fracture Accompanying Osteopenia : A Comparative Study
- Decision of Posterior Fixation Level by Load-Sharing Classification in Thoracolumbar and Lumbar Burst Fracture
- One Stage Decompression and Circumferential Stabilization by Posterior Approach in the Unstable Burst Fracture of Thoracolumbar and Lumbar Spine
- Comparison of Posterior Fixation Alone and Supplementation with Posterolateral Fusion in Thoracolumbar Burst Fractures
