High field strength magnetic resonance imaging in children
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. hwgoo@amc.seoul.kr
- KMID: 2064725
- DOI: http://doi.org/10.5124/jkma.2010.53.12.1093
Abstract
- Thanks to the benefits of 3 tesla (T) magnetic resonance imaging (MRI), its clinical use is increasing in pediatric patients. However, technical considerations and clinical applications of 3T MRI have not been comprehensively reviewed. Potential advantages of 3T imaging over 1.5T imaging include a higher signal-to-noise ratio, higher contrast-to-noise ratio, higher spatial resolution, and shorter scan time. These merits are easily achieved in neuroimaging, musculoskeletal imaging, and pelvic imaging, while body imaging is substantially limited by dielectric shading and an increased specific absorption rate (SAR) owing to B1 inhomogeneity and increased susceptibility artifacts. T1 and T2 relaxation times as well as chemical shifts are influenced by the higher magnetic field strength. SAR issues and dielectric shading of 3T body MRI are less problematic in pediatric patients having a smaller body size. Improved image quality can be achieved by using parallel imaging, the shortest echo time or echo train length, the highest receiver bandwidth, and improved local shimming. Potential reduction of scan time at 3T should be emphasized for pediatric patients. Three-dimensional MRI with post-processing can improve the image quality in a short acquisition time and, therefore, has become a clinical reality at 3T. A dual-source parallel radiofrequency excitation system can reduce dielectric shading, SAR, and scan time by increasing B1 homogeneity, which eventually improves the image quality of 3T body MRI. The usefulness of 3T MRI in pediatric patients can be maximized by further technical developments and optimization.
MeSH Terms
Figure
-
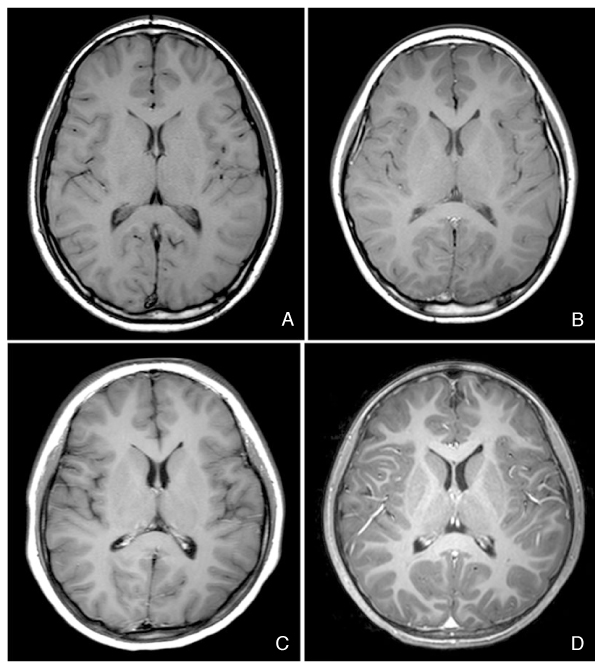
Figure 1 Axial T1-weighted brain magnetic resonance (MR) images. Compared with a spin-echo image (repetition time msec/echo time msec, 543.8/15.0; flip angle, 90°) at 1.5 tesla (T) (A), the signal-to-noise ratio of spin-echo image (500.0/10.0, 70°) at 3T (B) is higher but T1 contrast at 3T (B) is not sufficiently high. (C) Inversion-recovery turbo spin-echo image (2000.0/20.0; 90°; inversion time msec, 1000.0) shows improved T1 contrast. (D) A three-dimensional gradient-echo image (9.9/4.6, 8°) reveals an excellent signal-to-noise ratio as well as T1 contrast. It should be noted that the effect of the contrast agent is best on a spinecho-image at 3T (not shown) among T1-weighted MR images.

Figure 2 Axial, fat-saturated, T2-weighted abdominal magnetic resonance image (repetition time msec/echo time msec, 1,495.2/80.0; flip angle, 90°) at 3 tesla demonstrates an area of signal loss (arrows), e.g., dielectric shading, in the left lobe of the liver resulting from B1 field inhomogeneity.
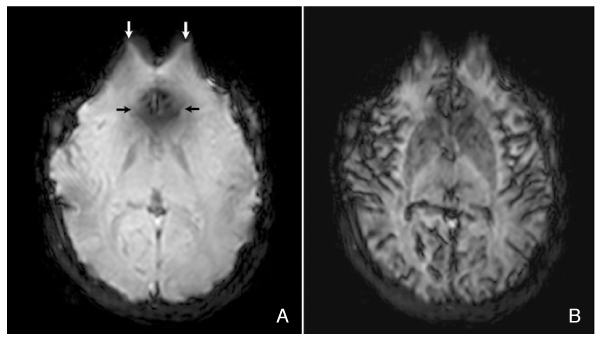
Figure 3 Axial T2*-weighted brain perfusion magnetic resonance (MR) images (repetition time msec/echo time msec, 1,779.2/40.0; flip angle, 90°) at 3 tesla. (A) Baseline image shows an area of signal loss (black arrows) and image distortion (white arrows) due to increased susceptibility at 3T. However, this increased susceptibility increases the T2* effect of contrast agent on T2*-weighted brain perfusion MR image (B).

Figure 4 Time-of-flight magnetic resonance (MR) angiography. Compared with MR angiography (repetition time msec/echo time msec, 25.0/3.0; flip angle, 20°) at 1.5 tesla (T) (A), MR angiography (25.0/3.5, 20°) at 3T (B) shows a much higher overall image quality. Thus, moyamoya vessels and prominent peripheral vessels (arrow) at the site of the left revascularization procedure are much better delineated on MR angiography at 3T (B).

Figure 5 Sagittal, fat-saturated, three-dimensional T2-weighted turbo spin-echo magnetic resonance image (repetition time msec/echo time msec, 3,000.0/155.5; flip angle, 90°) at 3 tesla (T) shows severe cerebrospinal fluid flow artifacts (arrows) in the posterior fossa and the cervical spinal canal.
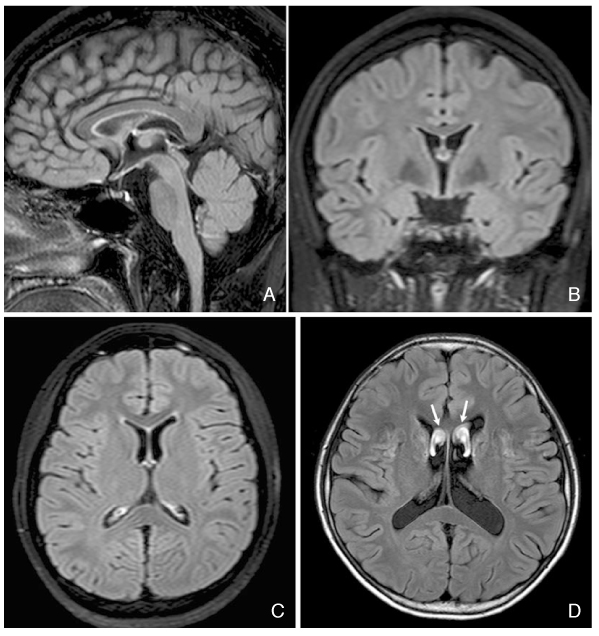
Figure 6 Fluid-attenuated inversion recovery (FLAIR) brain magnetic resonance (MR) images. Contrast-enhanced three-dimensional FLAIR 3 tesla (T) images (repetition time msec/echo time msec, 8,000.0/258.6; flip angle, 90°; 2,400.0) are acquired in the sagittal plane (A). Thanks to the almost isotropic feature of MR data, coronal (B) and axial (C) reformatted FLAIR images show comparable spatial resolution. Cerebrospinal fluid flow artifacts are entirely absent on three dimensional FLAIR images at 3T (A-C). In contrast, prominent cerebrospinal fluid flow artifacts (arrows) are often seen on two-dimensional FLAIR images (11,000.0/125.0; 90°; 2,800.0) at 3T (D).
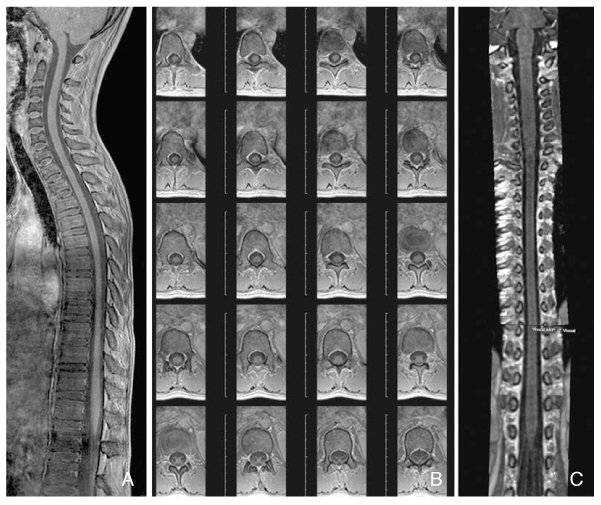
Figure 7 Three-dimensional spine magnetic resonance images (repetition time msec/echo time msec, 7.0/4.6; flip angle, 10°) at 3 tesla. The sagittal imaging plane is usually used to minimize the scan time. (A) A sagittal image of the whole spinal cord shows a high signal-to-noise ratio and high spatial resolution. In addition, the imaging technique not only provides seamless axial coverage of the whole spinal cord with reduced cerebrospinal fluid flow artifacts (B), but also facilitates various image reformations (C). In contrast, three-dimensional acquisition is susceptible to motion artifacts, particularly in the thoracic and abdominal regions (A), and may not be optimal to demonstrate marrow abnormalities.

Figure 8 Axial single-shot T1-weighted (repetition time msec/echo time msec, 15.0/4.6; flip angle, 15°) (A) and T2-weighted (15,000.0/90.0, 90°) (B) brain magnetic resonance images offer a faster scan time (approximately 30 seconds for the whole brain) and fewer motion artifacts.
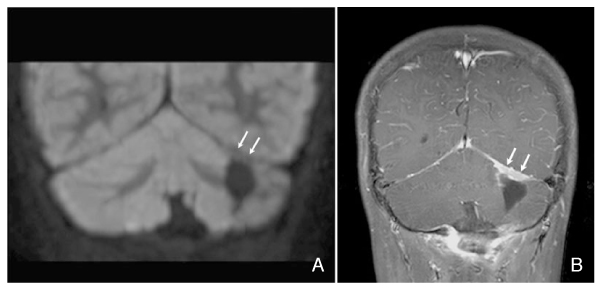
Figure 9 Diffusion-weighted imaging with background body signal suppression (DWIBS) (repetition time msec/echo time msec, 4,441.5/69.0; flip angle, 90°; b values s/mm2, 0 and 800) as an alternative to the usual diffusion-weighted imaging to reduce susceptibility artifacts. Coronal reformatted DWIBS brain magnetic resonance (MR) image (A) reveals the lack of restricted water diffusion in the plaque-like enhancing lesion (arrows) along the upper resection margin of medulloblastoma on coronal, fat-saturated, contrast-enhanced T1-weighted MR image (B), without susceptibility artifacts and image distortion.
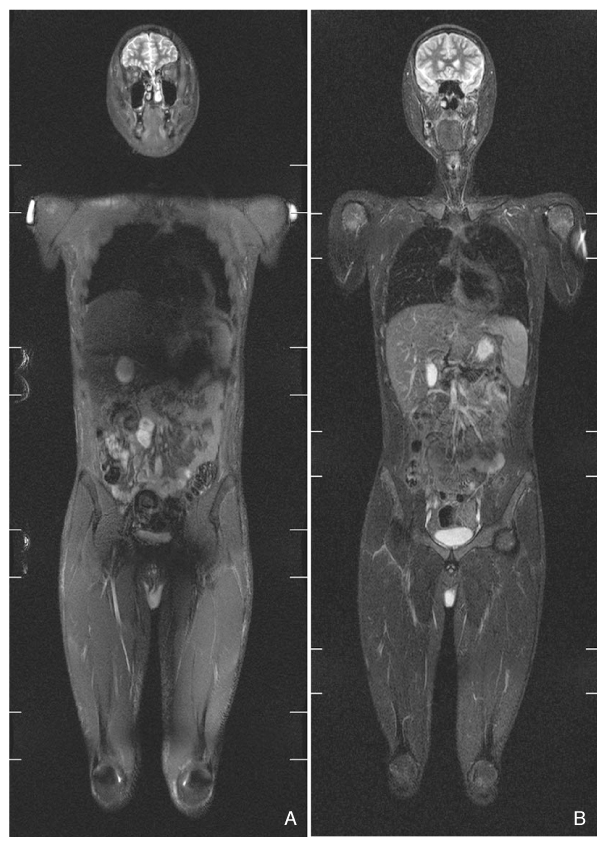
Figure 10 Whole-body magnetic resonance imaging. A coronal whole-body short tau inversion recovery (STIR) 3 tesla (T) image (A) (repetition time msec/echo time msec, 5,190.3/60.0; flip angle, 90°; 220,0) shows dielectric shading artifacts in the central portion of the upper abdomen and the groin. In contrast, a coronal whole-body STIR 1.5T image (B) (2,500.0/71.0; 90°; 160.0) demonstrates better image quality without dielectric shading.
Reference
-
1. Chavhan GB, Babyn PS, Singh M, Vidarsson L, Shroff M. MR imaging at 3.0 T in children: technical differences, safety issues, and initial experience. Radiographics. 2009. 29:1451–1466.
Article2. Dagia C, Ditchfield M. 3T MRI in paediatrics: challenges and clinical applications. Eur J Radiol. 2008. 68:309–319.
Article3. Kuhl CK, Träber F, Schild HH. Whole-body high-field-strength (3.0-T) MR Imaging in clinical practice. Part I. Technical considerations and clinical applications. Radiology. 2008. 246:675–696.
Article4. Kuhl CK, Träber F, Gieseke J, Drahanowsky W, Morakkabati-Spitz N, Willinek W, von Falkenhausen M, Manka C, Schild HH. Whole-body high-field-strength (3.0-T) MR imaging in clinical practice. Part II. Technical considerations and clinical applications. Radiology. 2008. 247:16–35.
Article5. Zimmerman RA, Bilaniuk LT, Pollock AN, Feygin T, Zarnow D, Schwartz ES, Harris C. 3.0 T versus 1.5 T pediatric brain imaging. Neuroimaging Clin N Am. 2006. 16:229–239.
Article6. Edelman RR, Dunkle E, Koktzoglou I, Griffin A, Russell EJ, Ankenbrandt W, Ragin A, Carrillo A. Rapid whole-brain magnetic resonance imaging with isotropic resolution at 3 Tesla. Invest Radiol. 2009. 44:54–59.
Article7. Chagla GH, Busse RF, Sydnor R, Rowley HA, Turski PA. Three-dimensional fluid attenuated inversion recovery imaging with isotropic resolution and nonselective adiabatic inversion provides improved three-dimensional visualization and cerebrospinal fluid suppression compared to two-dimensional flair at 3 tesla. Invest Radiol. 2008. 43:547–551.
Article8. Barth MM, Smith MP, Pedrosa I, Lenkinski RE, Rofsky NM. Body MR imaging at 3.0 T: understanding the opportunities and challenges. Radiographics. 2007. 27:1445–1462.
Article9. Wieben O, Francois C, Reeder SB. Cardiac MRI of ischemic heart disease at 3 T: potential and challenges. Eur J Radiol. 2008. 65:15–28.
Article10. Schmidt GP, Wintersperger B, Graser A, Baur-Melnyk A, Reiser MF, Schoenberg SO. High-resolution whole-body magnetic resonance imaging applications at 1.5 and 3 Tesla: a comparative study. Invest Radiol. 2007. 42:449–459.
Article11. Goo HW. Whole-body MRI of neuroblastoma. Eur J Radiol. 2010. 75:306–314.
Article12. Willinek WA, Gieseke J, Kukuk GM, Nelles M, König R, Morakkabati-Spitz N, Träber F, Thomas D, Kuhl CK, Schild HH. Dual-source parallel radiofrequency excitation body MR imaging compared with standard MR imaging at 3.0 T: initial clinical experience. Radiology. 2010. 256:966–975.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- High field strength magnetic resonance imaging of cardiovascular diseases
- Introduction to high field strength magnetic resonance imaging
- Clinical application of high field strength magnetic resonance imaging
- Review of Recent Advancement of Ultra High Field Magnetic Resonance Imaging: from Anatomy to Tractography
- High field strength magnetic resonance imaging of abdominal diseases
