Assessment on the Potential Role of Applying Cryoprobe for Tissue Ablation
- Affiliations
-
- 1Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. ytjeen@korea.ac.kr
- 2Department of Pathology, Korea University College of Medicine, Seoul, Korea.
- KMID: 2048834
- DOI: http://doi.org/10.5946/ce.2012.45.1.67
Abstract
- BACKGROUND/AIMS
Cryotherapy is the therapeutic application for tissue ablation. Clinical applications of cryotherpy such as in pulmonology have increased. Until now, its development in gastroenterology has been insignificant. But, as clinical application such as mucosal ablation on Barrett's esophagus became possible, various applications have been developed. Therefore, it is important to make standards of tissue injury's extent in cryotherapy prior to clinical trial. We evaluated the tissue injury according to the application of cryoprobe with a pig model.
METHODS
Cryoprobe was applied to several different segments of the esophagus and stomach for various lengths of time using various number of probe's contact in a pig model. After 48 hours, esophagus and stomach were harvested and histological tissue injury was assessed. The extent of tissue injury was decided by the injury of the deepest layer.
RESULTS
Endoscopic application of cryoprobe on esophagus and stomach resulted in a dose-dependent injury: esophageal necrosis was limited to the submucosa after 10 seconds of cryotherapy, and extended to involve the transmural necrosis after over 15 seconds. Necrosis on stomach was extended to involve the transmural necrosis after over 20 seconds.
CONCLUSIONS
Positive relationship was seen between the duration and frequency of cryoprobe application and the extent of tissue injury.
Keyword
Figure
-
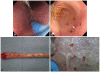
Fig. 1 Cryoablation of pig's upper gastrointestinal tract. (A) Cryoablation by cryoprobe near endocliping site on esophagus. (B) Mucosal lesion after cryoablation on stomach. (C) Surgically resected esophagus after 48 hours. (D) Surgically resected stomach after 48 hours.

Fig. 2 Histopathologic findings of various durations of esophageal cryotherapy (H&E stain, ×100). (A) Cryoablation for 10 seconds, necrosis involving the layers of mucosa and submucosa but not muscularis propria. (B) Cryoablation for 15 seconds, attenuated surface epithelium, necrotic lamina propria and muscularis mucosa and inflammatory extension to focal muscularis propria. (C) Cryoablation for 20 seconds, necrosis and inflammatory reaction involving the submucosa and extension to the muscularis propria. (D) Cryoablation for 30 seconds, necrosis and edema involving the layers of submucosa and the mucularis propria.

Fig. 3 Histopathologic findings of various durations of gastric cryotherapy (H&E stain, ×100). (A) Cryoablation for 10 seconds, loss of upper part of mucosa and focal necrosis in the deeper part of mucosa, but not in other layers. (B) Cryoablation for 20 seconds, necrosis and inflammatory reaction in the submucosal layer. (C) Cryoablation for 10 seconds twice, loss and necrosis involving the layers of mucosa and submucosa and slight extension to superfical part of muscularis propria. (D) Cryoablation for 60 seconds, necrosis in the submucosal layer and extension to muscularis propria.

Fig. 4 Effect of increasing duration of esophageal cryotherapy on the transmural extent of necrosis. Grade 0, no necrosis; Grade 1, necrosis involving mucosa only; Grade 2, necrosis involving submucosa; Grade 3, necrosis involving muscularis propria; Grade 4, transmural necrosis.

Fig. 5 Effect of increasing duration of gastric cryotherapy on the transmural extent of necrosis. Grade 0, no necrosis; Grade 1, necrosis involving mucosa only; Grade 2, necrosis involving submucosa; Grade 3, necrosis involving muscularis propria; Grade 4, transmural necrosis.
Reference
-
1. American Society for Gastrointesstinal Endoscopy Technology Committee. Mucosal ablation devices. Gastrointest Endosc. 2008; 68:1031–1042. PMID: 19028211.2. Sguazzi A, Bracco D. A historical account of the technical means used in cryotherapy. Minerva Med. 1974; 65:3718–3722. PMID: 4609141.3. Cooper IS. Cryobiology as viewed by the surgeon. Cryobiology. 1964; 51:44–51. PMID: 14247541.
Article4. Shaheen NJ, Greenwald BD, Peery AF, et al. Safety and efficacy of endoscopic spray cryotherapy for Barrett's esophagus with high-grade dysplasia. Gastrointest Endosc. 2010; 71:680–685. PMID: 20363409.
Article5. Kantsevoy SV, Cruz-Correa MR, Vaughn CA, Jagannath SB, Pasricha PJ, Kalloo AN. Endoscopic cryotherapy for the treatment of bleeding mucosal vascular lesions of the GI tract: a pilot study. Gastrointest Endosc. 2003; 57:403–406. PMID: 12612530.
Article6. Kaouk JH, Aron M, Rewcastle JC, Gill IS. Cryotherapy: clinical end points and their experimental foundations. Urology. 2006; 68(1 Suppl):38–44. PMID: 16857458.
Article7. Franke KJ, Szyrach M, Nilius G, et al. Experimental study on biopsy sampling using new flexible cryoprobes: influence of activation time, probe size, tissue consistency, and contact pressure of the probe on the size of the biopsy specimen. Lung. 2009; 187:253–259. PMID: 19548030.
Article8. Maiwand MO, Homasson JP. Cryotherapy for tracheobronchial disorders. Clin Chest Med. 1995; 16:427–443. PMID: 8521698.
Article9. Raju GS, Ahmed I, Xiao SY, Brining D, Bhutani MS, Pasricha PJ. Graded esophageal mucosal ablation with cryotherapy, and the protective effects of submucosal saline. Endoscopy. 2005; 37:523–526. PMID: 15933923.
Article10. Chino A, Karasawa T, Uragami N, Endo Y, Takahashi H, Fujita R. A comparison of depth of tissue injury caused by different modes of electrosurgical current in a pig colon model. Gastrointest Endosc. 2004; 59:374–379. PMID: 14997134.
Article11. Gage AA, Baust J. Mechanisms of tissue injury in cryosurgery. Cryobiology. 1998; 37:171–186. PMID: 9787063.
Article12. Sheski FD, Mathur PN. Cryotherapy, electrocautery, and brachytherapy. Clin Chest Med. 1999; 20:123–138. PMID: 10205722.
Article13. Whittaker DK. Repeat freeze cycles in cryosurgery of oral tissues. Br Dent J. 1975; 139:459–465. PMID: 1060465.
Article14. Rubinsky B, Ikeda M. A cryomicroscope using directional solidification for the controlled freezing of biological material. Cryobiology. 1985; 22:55–68.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Irreversible electroporation of hepatocellular carcinoma: the role of ultrasonography
- Efficacy of Cox Maze IV Procedure Using Argon-Based Cryoablation: A Comparative Study with N2O-Based Cryoablation
- Excimer Laser Tissue Ablation: The Potential Role of Laser Induced Shock Waves and Problems Associated with Contact Dependent Multifiber Laser Catheter
- A Clinical Case of the Extensive Tissue Necrosis Due to Radiofrequency Ablation Applied on Malignant Melanoma
- Efficacy of Foreign Body Removal using a Cryoprobe in Flexible Bronchoscopy
