Multiple Cardiovascular Manifestations in a Patient with Autosomal Dominant Polycystic Kidney Disease
- Affiliations
-
- 1Department of Internal Medicine, Gyeongsang National University Hospital, Gyeongsang National University School of Medicine, Jinju, Korea. park-jr@nate.com
- KMID: 2045431
- DOI: http://doi.org/10.4250/jcu.2014.22.3.144
Abstract
- Autosomal dominant polycystic kidney disease (ADPKD) is a systemic disorder associated with various extrarenal complications. The major cardiovascular complications of ADPKD include valvulopathies and vascular ectasia. A 64-year-old man who was diagnosed with ADPKD seven years previously was admitted to our hospital for heart failure. Pelvic computed tomography revealed multiple variable-sized cysts in both kidneys. Transthoracic echocardiography showed enlargement of the left ventricle and left atrium. Severe mitral regurgitation and moderate aortic regurgitation with annuloaortic ectasia were observed. The left main coronary artery was dilated. The patient had various cardiovascular features associated with ADPKD.
MeSH Terms
Figure
-
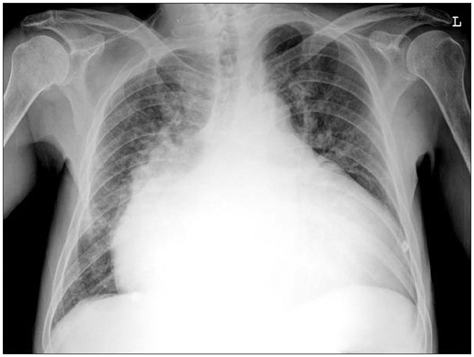
Fig. 1 Initial chest radiography. Chest radiography shows severe cardiomegaly and pulmonary congestion in both lung fields.
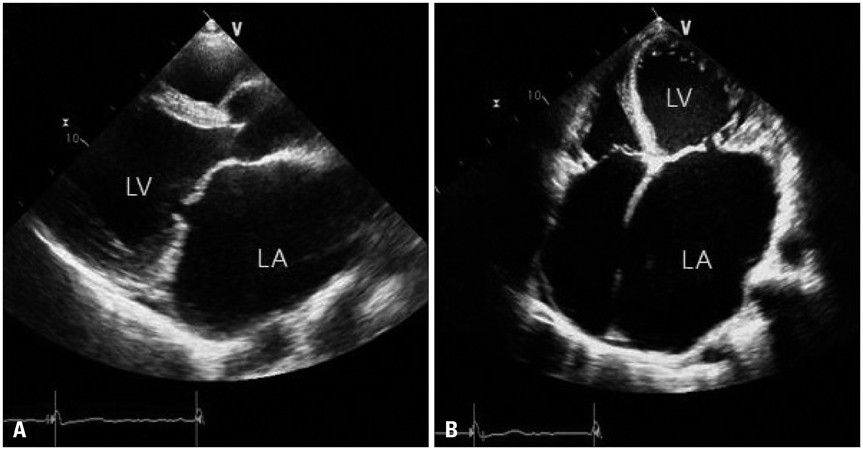
Fig. 2 Two-dimensional echocardiography. The left ventricular end-diastolic dimension/body surface area was approximately 44 mm/m2 and the left atrial volume index was calculated to be approximately 614 mL/m2 by the area-length method. Tethering and malcoaptation of the mitral valve are observed at end diastole. A: Parasternal long-axis view. B: Apical four-chamber view. LA: left atrium, LV: left ventricle.
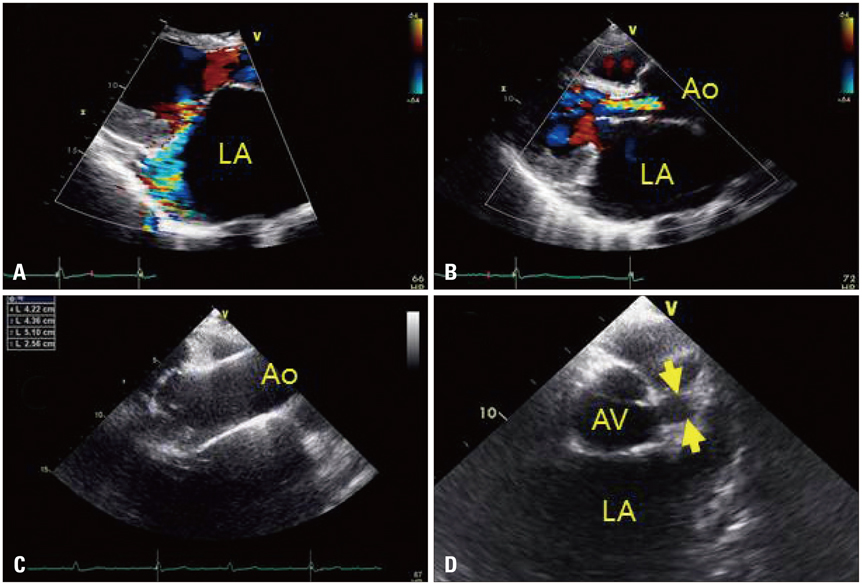
Fig. 3 Transthoracic echocardiography. A: Eccentric and severe mitral regurgitation is observed on the parasternal long-axis view. B: Moderate aortic regurgitation is shown on the parasternal long-axis view. The size of the vena contracta is approximately 6 mm. C: The modified parasternal long-axis view shows annuloaortic ectasia. D: At the aortic valve level of the parasternal short-axis view, 15-mm dilatation of the left main coronary artery (arrows) is seen. LA: left atrium, Ao: aorta, AV: aortic valve.
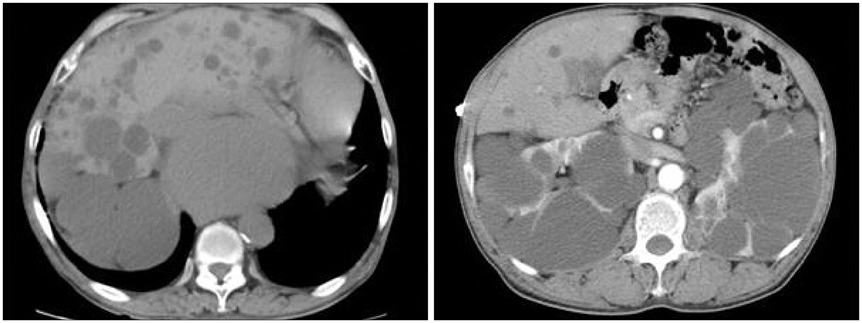
Fig. 4 Abdominal computed tomography. Abdominal enhanced computed tomography shows multiple variable-sized cysts in both the kidney and liver. The abdominal aorta and branches are normal.
Reference
-
1. Gabow PA. Autosomal dominant polycystic kidney disease. N Engl J Med. 1993; 329:332–342.
Article2. Perrone RD. Extrarenal manifestations of ADPKD. Kidney Int. 1997; 51:2022–2036.
Article3. Hossack KF, Leddy CL, Johnson AM, Schrier RW, Gabow PA. Echocardiographic findings in autosomal dominant polycystic kidney disease. N Engl J Med. 1988; 319:907–912.
Article4. Leier CV, Baker PB, Kilman JW, Wooley CF. Cardiovascular abnormalities associated with adult polycystic kidney disease. Ann Intern Med. 1984; 100:683–688.
Article5. Hadimeri H, Lamm C, Nyberg G. Coronary aneurysms in patients with autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1998; 9:837–841.
Article6. Basile C, Lucarelli K, Langialonga T. Spontaneous coronary artery dissection: one more extrarenal manifestation of autosomal dominant polycystic kidney disease? J Nephrol. 2009; 22:414–416.7. Helal I, Reed B, Mettler P, Mc Fann K, Tkachenko O, Yan XD, Schrier RW. Prevalence of cardiovascular events in patients with autosomal dominant polycystic kidney disease. Am J Nephrol. 2012; 36:362–370.
Article8. Lumiaho A, Ikäheimo R, Miettinen R, Niemitukia L, Laitinen T, Rantala A, Lampainen E, Laakso M, Hartikainen J. Mitral valve prolapse and mitral regurgitation are common in patients with polycystic kidney disease type 1. Am J Kidney Dis. 2001; 38:1208–1216.
Article9. Torres VE, Harris PC. Autosomal dominant polycystic kidney disease: the last 3 years. Kidney Int. 2009; 76:149–168.
Article10. Kim J, Kim SM, Lee SY, Lee HC, Bae JW, Hwang KK, Kim DW, Cho MC, Byeon SJ, Kim KB. A case of severe aortic valve regurgitation caused by an ascending aortic aneurysm in a young patient with autosomal dominant polycystic kidney disease and normal renal function. Korean Circ J. 2012; 42:136–139.
Article11. Paavola J, Schliffke S, Rossetti S, Kuo IY, Yuan S, Sun Z, Harris PC, Torres VE, Ehrlich BE. Polycystin-2 mutations lead to impaired calcium cycling in the heart and predispose to dilated cardiomyopathy. J Mol Cell Cardiol. 2013; 58:199–208.
Article12. Choe SC, Jeon ES, Hwang SD. A case of dilated cardiomyopathy associated with autosomal dominant polycystic kidney disease. J Korean Soc Echocardiogr. 2001; 9:152–156.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Dilated Cardiomyopathy Associated with Autosomal Dominant Polycystic Kidney Disease
- A Case of Renal Cell Carcinoma in Autosomal Dominant Polycystic Kidney Disease Hemodialyzed
- Autosomal Dominant Polycystic Kidney Desease Coexisting with Renal Dysplasia. First Case Described and Followed Since Prenatal Period
- A Case of ESRD Caused by ADPKD (Autosomal Dominant Polycystic Kidney Disease) in a 17-year-old Patient
- Segmental Cystic Disease of the Kidney: A Case Report
