Diffusion-Weighted MR Imaging of Upper Abdomen: Comparison of Breath-Hold, Free-Breathing, and Respiratory-Triggered Techniques
- Affiliations
-
- 1Department of Radiology and the Research Institute of Radiological Science, Yonsei University College of Medicine, Gangnam Severance Hospital, Korea. yjsrad97@yuhs.ac
- KMID: 2040815
- DOI: http://doi.org/10.3348/jksr.2011.64.5.465
Abstract
- PURPOSE
To compare the image quality and stability of apparent diffusion coefficient (ADC) in diffusion-weighted MRI (DWI) of the upper abdomen among the breath-hold (BH), free-breathing (FB) and respiratory-triggered (RT) techniques.
MATERIALS AND METHODS
We analyzed the qualitative and quantitative parameters of 204 consecutive patients who underwent DWI (BH-DWI, FB-DWI or RT-DWI; n=68 in each technique). Qualitative parameters included liver contour, vascular landmarks, intra-slice homogeneity, and inter-slice discontinuity on DWI with a b-factor of 800 s/mm2 and a four-grade scale. Quantitative parameters included inter-slice or intraslice inhomogeneity of ADC in the spleen.
RESULTS
RT-DWI showed better liver contour compared to BH-DWI (p < 0.001) or FB-DWI (p = 0.001). As for the quality of the vascular landmarks, BH-DWI was inferior to FB-DWI (p = 0.025) and RT-DWI (p < 0.001). FB-DWI had the poorest result (p < 0.001) for inter-slice discontinuity compared to the other techniques. FB-DWI showed significantly larger inter-slice differences between the highest and the lowest ADCs in the spleen compared with those of RT-DWI (p < 0.001). Intra-slice homogeneity was significantly better in RT-DWI and FB-DWI than in BH-DWI (p < 0.001).
CONCLUSION
Compared with BH or FB techniques, RT-DWI appears to result in the best imaging by providing better anatomic detail without skipping continuous slices, in addition to more homogeneous ADCs.
MeSH Terms
Figure
-
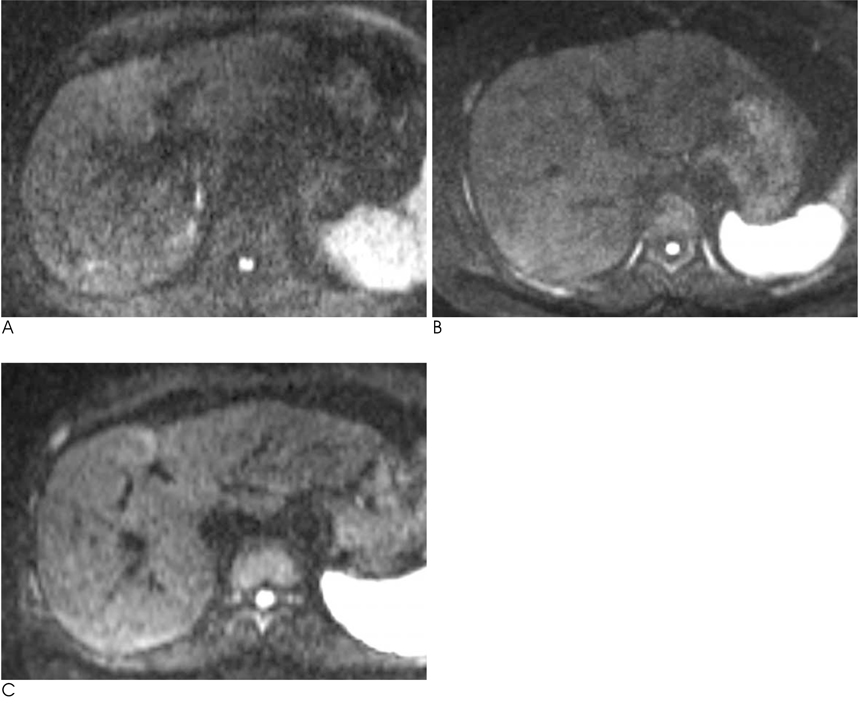
Fig. 1 Representative examples of diffusion-weighted MR images of b=800 mm2/s with breath-hold, free-breathing, and respiratory-triggered methods in three different patients. A-C. Vascular landmarks are poorer on breath-hold image (A) due to the lower signal-to-noise ratio compared to the free-breathing (B) or respiratory-triggered images (C). Respiratory-triggered imaging (C) shows better overall image quality in the liver contour, especially for the left lobe, when compared to the other images.
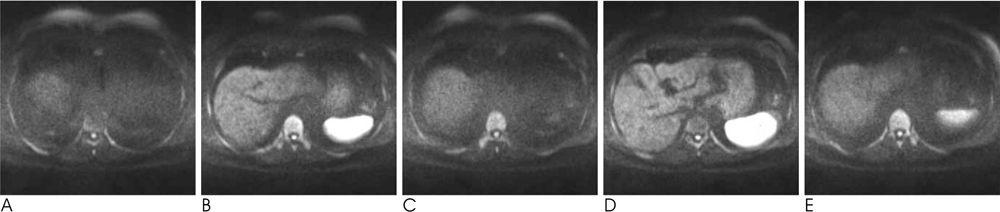
Fig. 2 A representative example of five contiguous slices of diffusion-weighted imaging (b=800 mm2/s) with use of the free-breathing technique in a 64-year-old man with a cirrhotic liver. A-E. From (A) to (E), the axial image slices are markedly discontinuous, passing around the liver dome to right hepatic vein level. The signal intensities of the hepatic parenchyma are not homogeneous between the slices due to a serious misregistration effect during the free-breathing.
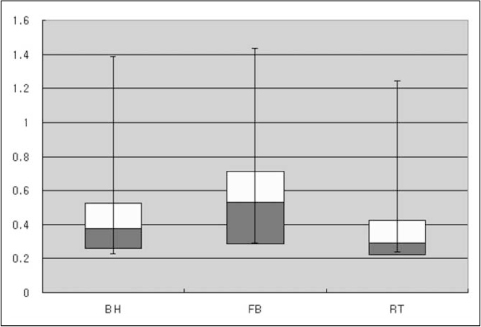
Fig. 3 Box-plots of mean inter-slice differences of apparent diffusion coefficients (ADCs) measured in the spleen on the three diffusion-weighted images of the breath-hold (BH), free-breathing (FB) and respiratory-triggered (RT) techniques. The decimal numbers on the y-axis are inter-slice differences of ADCs (×10-3 mm2/s). FB shows a significantly greater interslice difference between the highest and lowest ADCs compared to RT.
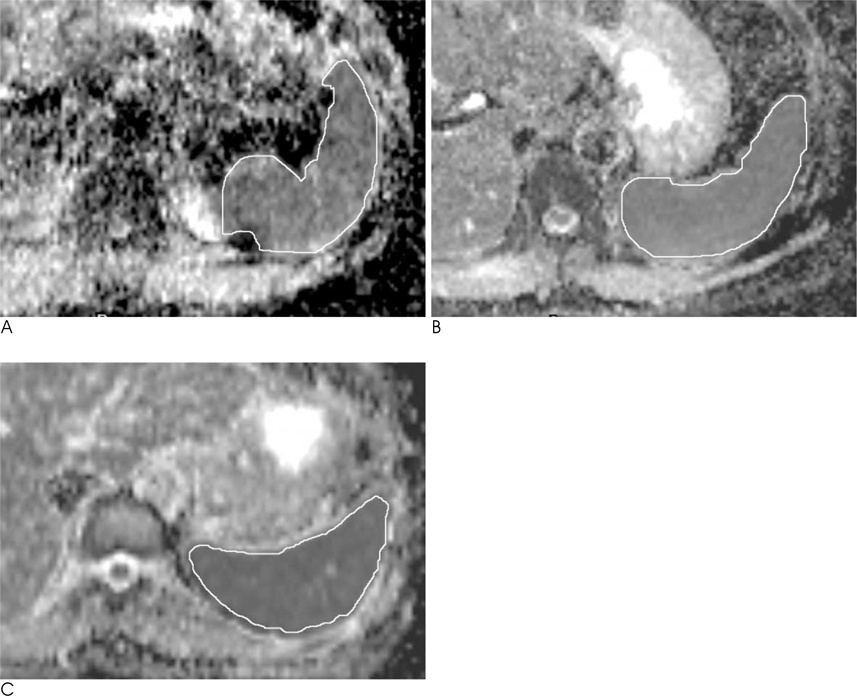
Fig. 4 A representative example of automatically calculated apparent diffusion coefficient (ADC) maps at the level of the maximum diameter of the spleens in three different patients. A-C. The region-of-interest is placed as the largest area possible in the spleen in each image by the breath-hold image (A), and shows largest standard deviation compared with free-breathing (B) or respiratory-triggered (C) images. The standard deviations of ADCs in the above images are as follows: breath-hold, 1.50×10-3 mm2/s; free-breathing, 0.88×10-3 mm2/s; respiratory-triggered, 0.93×10-3mm2/s.
Reference
-
1. Ichikawa T, Haradome H, Hachiya J, Nitatori T, Araki T. Diffusion-weighted MR imaging with a single-shot echoplanar sequence: detection and characterization of focal hepatic lesions. AJR Am J Roentgenol. 1998; 170:397–402.2. Nasu K, Kuroki Y, Nawano S, et al. Hepatic metastases: diffusion-weighted sensitivity-encoding versus SPIO-enhanced MR imaging. Radiology. 2006; 239:122–130.3. Kim T, Murakami T, Takahashi S, Hori M, Tsuda K, Nakamura H. Diffusion-weighted single-shot echoplanar MR imaging for liver disease. AJR Am J Roentgenol. 1999; 173:393–398.4. Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J, Laval-Jeantet M. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology. 1988; 168:497–505.5. Stejskal EO, Tanner JE. Spin diffusion measurements: spin-echo in the presence of a time dependent field gradient. J Chem Phys. 1962; 42:288–292.6. Naganawa S, Kawai H, Fukatsu H, Sakurai Y, Aoki I, Miura S, et al. Diffusion-weighted imaging of the liver: technical challenges and prospects for the future. Magn Reson Med Sci. 2005; 4:175–186.7. Kandpal H, Sharma R, Madhusudhan KS, Kapoor KS. Respiratory-triggered versus breath-hold diffusion-weighted MRI of liver lesions: comparison of image quality and apparent diffusion coefficient values. AJR Am J Roentgenol. 2009; 192:915–922.8. Kwee TC, Takahara T, Koh DM, Nievelstein RA, Luijten PR. Comparison and reproducibility of ADC measurements in breath-hold, respiratory triggered, and free-breathing diffusion-weighted MR imaging of the liver. J Magn Reson Imaging. 2008; 28:1141–1148.9. Taouli B, Koh DM. Diffusion-weighted MR imaging of the liver. Radiology. 2010; 254:47–66.10. Koh DM, Collins DJ. Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol. 2007; 188:1622–1635.11. Charles-Edwards EM, deSouza NM. Diffusion-weighted magnetic resonance imaging and its application to cancer. Cancer Imaging. 2006; 6:135–143.12. Koh DM, Takahara T, Imai Y, Collins DJ. Practical aspects of assessing tumors using clinical diffusion-weighted imaging in the body. Magn Reson Med Sci. 2007; 6:211–224.13. Takahara T, Imai Y, Yamashita T, Yasuda S, Nasu S, van Cauteren M. Diffusion weighted whole body imaging with background body signal suppression (DWIBS): technical improvement using free breathing, STIR and high resolution 3D display. Radiat Med. 2004; 22:275–282.14. Asbach P, Hein PA, Stemmer A, Wagner M, Hyppertz A, Hamm B, et al. Free-breathing echo-planar imaging based diffusion-weighted magnetic resonance imaging of the liver with prospective acquisition correction. J Comput Assist Tomogr. 2008; 32:372–378.15. Nasu K, Kuroki Y, Sekiguchi R, Nawano S. The effect of simultaneous use of respiratory triggering in diffusion-weighted imaging of the liver. Magn Reson Med Sci. 2006; 5:129–136.16. Nasu K, Kuroki Y, Fujii H, Minami M. Hepatic pseudo-anisotropy: a specific artifact in hepatic diffusion-weighted images obtained with respiratory triggering. MAGMA. 2007; 20:205–211.17. Kim SY, Lee SS, Byun JH, et al. Malignant hepatic tumors: short-term reproducibility of apparent diffusion coefficients with breath-hold and respiratory-triggered diffusion weighted MR imaging. Radiology. 2010; 255:815–823.18. Kim T, Murakami T, Takahashi S, Hori M, Tsuda K, Nakamura H. Diffusion-weighted single-shot echoplanar MR imaging for liver disease. AJR Am J Roentgenol. 1999; 173:393–398.19. Müller MF, Prasad P, Siewert B, Nissenbaum MA, Raptopoulos V, Edelman RR. Abdominal diffusion mapping with use of a whole-body echo-planar system. Radiology. 1994; 190:475–458.20. Weih KS, Driesel W, von Mengershausen M, Norris DG. Online motion correction for diffusion-weighted segmented-EPI and FLASH imaging. MAGMA. 2004; 16:277–283.21. Deng J, Omary RA, Larson AC. Multishot diffusion-weighted SPLICE PROPELLER MRI of the abdomen. Magn Reson Med. 2008; 59:947–953.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Detection of Hepatic Lesion: Comparison of Free-Breathing and Respiratory-Triggered Diffusion-Weighted MR imaging on 1.5-T MR system
- MR Cholangiopancreatography: Comparison of Breath-hold Fast Spin Echo and Respiratory Triggered Fast Spin Echo Techniques
- Quasi-breath-hold (QBH) Biofeedback in Gated 3D Thoracic MRI: Feasibility Study
- Comparison of Non-Breath-Hold T2-weighted Turbo Spin-Echo and Three Breath-Hold T2-weighted MR Images for Detection of Focal Hepatic Lesion
- Optimal MR Pulse Sequences for Hepatic Hemangiomas: Comparison of T2-Weighted Turbo-Spin-Echo, T2-Weighted Breath-hold Turbo-Spin-Echo, and T1-Weighted FLASH Dynamic Imaging
