A Case of Stress-Induced Cardiomyopathy Related with the Postpartum Period
- Affiliations
-
- 1Division of Cardiology, College of Medicine, The Catholic University of Korea, Daejeon St. Mary's Hospital, Daejeon, Korea. hhhsungho@naver.com
- KMID: 2029068
- DOI: http://doi.org/10.4070/kcj.2007.37.8.388
Abstract
- Stress-induced cardiomyopathy is a relatively rare, unique entity that has only recently been widely appreciated. It characterized by transient left ventricular regional wall motion abnormalities (with a peculiar apical ballooning appearance), chest pain or dyspnea, ST-segment elevation and/or T wave inversion and minor elevations of the cardiac enzyme levels. The patients in the previous series were usually women over 50 years of age and a triggering event was identified in most cases; these included severe emotional distress or an acute medical illness. Although reports of single episodes of stress-induced cardiomyopathy are not infrequent in the recent medical literature, we report here on a case of stress-induced cardiomyopathy in a young women, and this was related with the post-partum period as a stressful condition.
Keyword
Figure
-

Fig. 1 Electrocardiogram in the primary clinic and the EMS ambulance before admission. A: the twelve-lead electrocardiogram done at the primary clinic revealed a normal sinus rhythm and a normal QT interval (corrected QT interval: 0.430 second). B: the rhythm strip demonstrating ventricular fibrillation. C: the rhythm strip taken during defibrillation by the EMS team. EMS: emergency medical service.
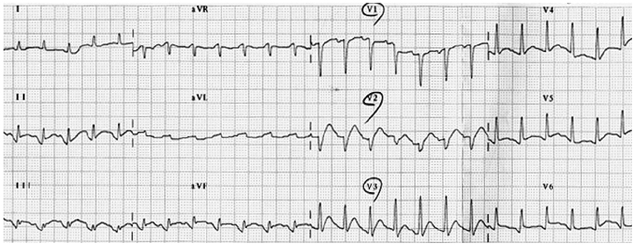
Fig. 2 The twelve-lead electrocardiogram obtained upon admission (post-resuscitation) depicts mild ST segment elevation in the II, III and aVF leads and in the V1-V6 leads.
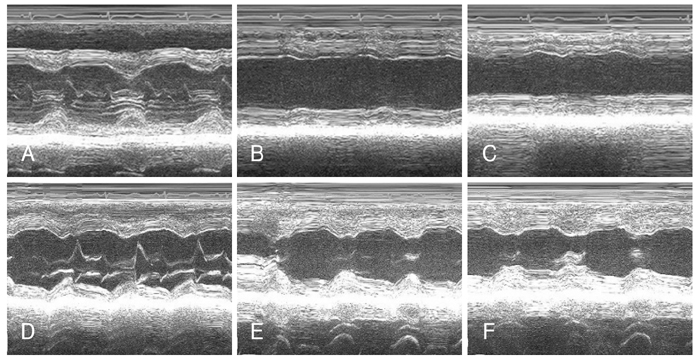
Fig. 3 Echocardiography depicts the reversible apical wall motion abnormality. A: the echocardiogram obtained upon admission depicts hyperkinesis of the basal segments, which was observed via the M-mode. B: hypokinesis of the mid-portion of the left ventricle was observed. C: hypokinesis of the apex was observed. D: echocardiograms taken 14 days after admission showed no interval change of the basal segment. E: improvement of the mid-ventricular wall motion was observed on the follow up echocardiograms. F: improvement of the apical wall motion is demonstrated.

Fig. 4 A: the left coronary artery in the cranial right anterior oblique and caudal views showing the coronary arteries with no obstructive lesions. B: a spasm provoked by ergonovine was observed in the left anterior descending artery. C: it was relieved by nitroglycerin.
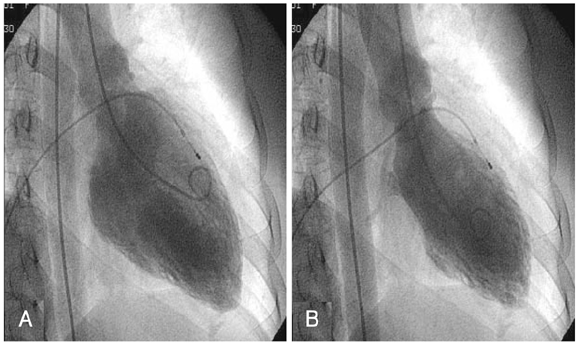
Fig. 5 Representative left ventriculogram from the patient: images obtained in diastole (A) and systole (B). Left ventriculography revealed akinesis of the left ventricular apex and the mid-portion.
Reference
-
1. Kawai S, Suzuki H, Yamaguchi H, et al. Ampulla cardiomyopathy (takotsubo cardiomyopathy): reversible left ventricular dysfunction with ST segment elevation. Jpn Circ J. 2000. 64:156–159.2. Kurisu S, Sato H, Kawagoe T, et al. Takotsubo like left ventricular dysfunction with ST-segment elevation: a novel cardiac syndrome mimicking acute myocardial infarction. Am Heart J. 2002. 143:448–455.3. Virani SS, Khan AN, Mendoza CE, Ferreira AC, de Marchena E. Takotsubo cardiomyopathy, or broken heart syndrome. Tex Heart Inst J. 2007. 34:76–79.4. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006. 27:1523–1529.5. Bybee KA, Kara T, Prasad A, et al. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med. 2004. 141:858–865.6. Lee HH, Gwon HC, Kim BJ, et al. Clinical manifestation of novel stress-induced cardiomyopathy mimicking acute myocardial infarction: single center prospective registry. Korean Circ J. 2002. 32:1054–1063.7. Sato M, Fujita S, Saito S, et al. Increased incidence of transient left ventricular apical ballooning (so-called "Takotsubo" cardiomypathy) after the mid-Niigata Prefecture earthquake. Circ J. 2006. 70:947–953.8. Cherian J, Angelis D, Filiberti A, Saperia G. Recurrence of stress-induced (takotsubo) cardiomyopathy. Cardiology. 2006. 108:144–146.9. Chang KY, Jeon HK, Chae JS, et al. A novel cardiomyopathy mimicking acute myocardial infarction. Korean Circ J. 2002. 32:608–612.10. Park JH, Kang SJ, Song JK, et al. Left ventricular apical ballooning due to severe physical stress in patients admitted to the medical ICU. Chest. 2005. 128:296–302.11. Tsuchihashi K, Ueshima K, Uchida T, et al. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. J Am Coll Cardiol. 2001. 38:11–18.12. Sharkey SW, Shear W, Hodges M, Herzog CA. Reversible myocardial contraction abnormalities in patients with an acute noncardiac illness. Chest. 1998. 114:98–105.13. Yamasa T, Ikeda S, Ninomiya A, et al. Characteristic clinical findings of reversible left ventricular dysfunction. Intern Med. 2002. 41:789–792.14. Mukoyama M, Nakao K, Saito Y, et al. Human brain natriuretic peptide: a novel cardiac hormone. Lancet. 1990. 335:801–802.15. Akashi YJ, Nakazawa K, Sakakibara M, Miyake F, Sasaka K. Reversible left ventricular dysfunction "takotsubo" cardiomyopathy related to catecholamine cardiotoxicity. J Electrocardiol. 2002. 35:351–356.16. Ako J, Kozaki K, Yoshizumi M, Ouchi Y. Transient left ventricular apical ballooning without coronary artery stenosis: a form of stunning-like phenomenon? J Am Coll Cardiol. 2002. 39:741–742.17. Kushiro T, Saito F, Kusama J, et al. Takotsubo shaped cardiomyopathy with type I CD36 deficiency. Heart Vessels. 2005. 20:123–125.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrent fetal postpartum stress induced cardiomyopathy after normal vaginal delivery
- Stress-induced Cardiomyopathy Following Cesarean Delivery with Hemorrhagic Shock: A Case Report
- A Case of Stress-induced Cardiomyopathyin Patient after Massive Postpartal Bleeding
- A Case of Postpartum Cardiomyopathy
- A case of stress-induced cardiomyopathy with an "inverted Takotsubo" contractile pattern
