The Changes of the Dimension of Intervertebral Disc,-Neural Foramen and Spinal Canal after Anterior Lumbar Interbody Fusion in the Lumbar Spine
- Affiliations
-
- 1Department of Orthopaedic Surgery, Ajou University School of Medicine, Korea.
- 2Department of Orthopedic Surgery, Konyang University School of Medicine, Korea. spinekyc@kyuh.co.kr
- KMID: 2003190
- DOI: http://doi.org/10.4184/jkss.2004.11.1.40
Abstract
- STUDY DESIGN: A prospective radiological assessment was conducted.
OBJECTIVES
To analyze the changes in the heights of the intervertebral disc and neural foramen, and the diameters and areas of the dural sac and lateral recess following anterior lumbar interbody fusion and posterior fixation in lumbar degenerative disease. SUMMARY OF LITERATURE REVIEW: Anterior lumbar interbody fusion distracts from the height of the intervertebral disc and neural foramen and increase the area of the spinal canal.
MATERIALS AND METHODS
A mini-open anterior lumbar interbody fusion and posterior fixation was performed on 40 cases between January 1999 and March 2002. The measured factors included the height of the intervertebral disc and neural foramen, the midsagittal and lateral diameters of the dural sac, the area of the dural sac and the diameter of the lateral recess. These were measured with calipers in 1mm reconstructive computed tomography images before and 6 months after the anterior lumbar interbody fusion. The measured factors were independently taken by three different orthopaedic surgeons.
RESULTS
The heights of the intervertebral disc and neural foramen were increased by means of 39.1 and 18.7% respectively. The midsagittal diameter of the dural sac was increased by a mean of 11.6% and that of the lateral dural sac decreased by a mean of 3.7%. The area of the dural sac was increased by a mean of 8.1% and the diameter of lateral recess by a mean of 26.3%. There were statistically significant increases in all the measured factors, with the exception of the lateral diameter of the dural sac.
CONCLUSIONS
Anterior lumbar interbody fusion significantly increases the heights of the intervertebral disc and neural foramen, the midsagittal diameter of the dural sac, the area of the dural sac and the diameter of the lateral recess, but not the lateral diameter of the dural sac.
Figure
-
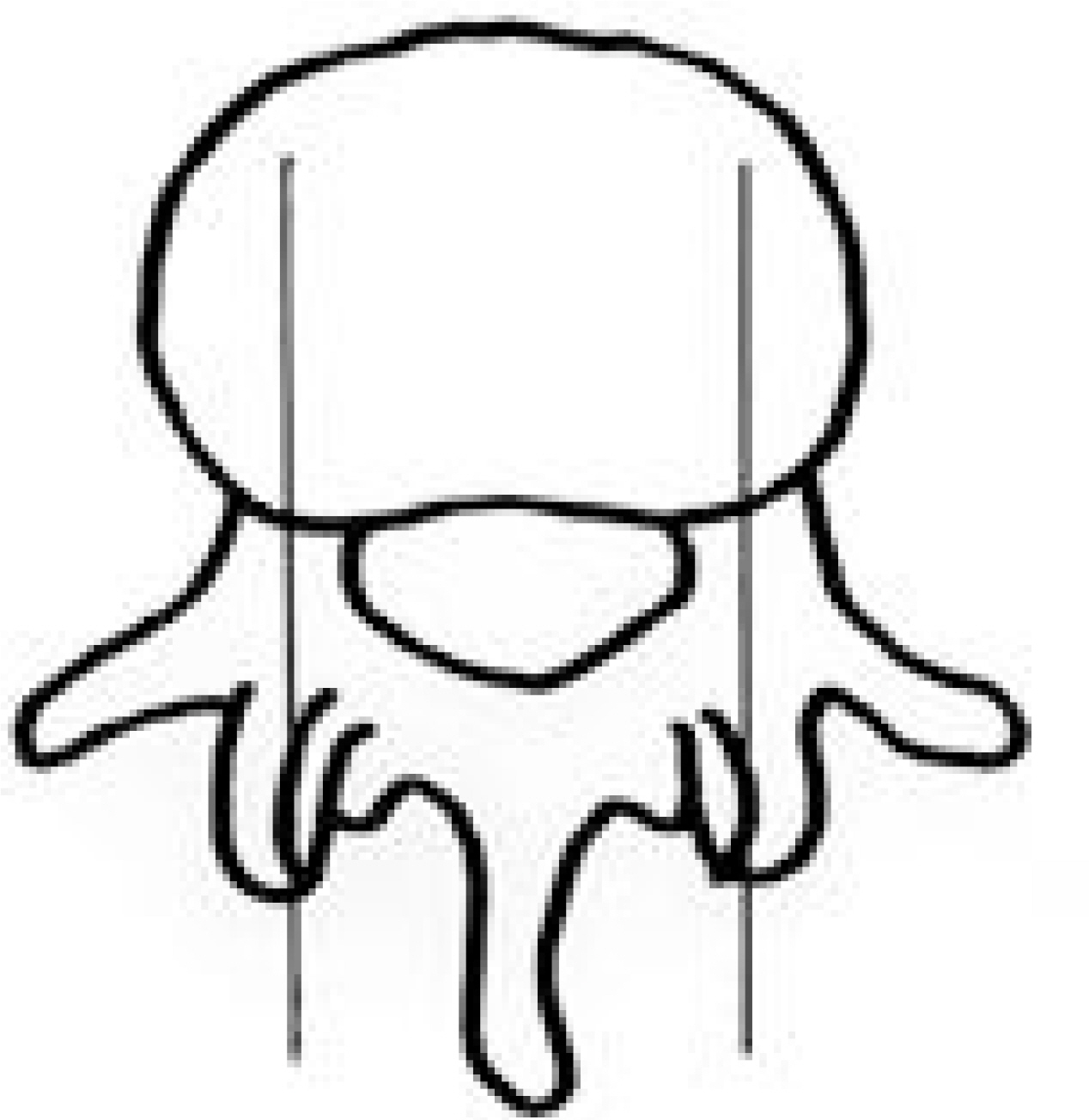
Fig. 1. CT measurement were done via sagittal reconstruction at the level of the mid pedicle on axial CT cut
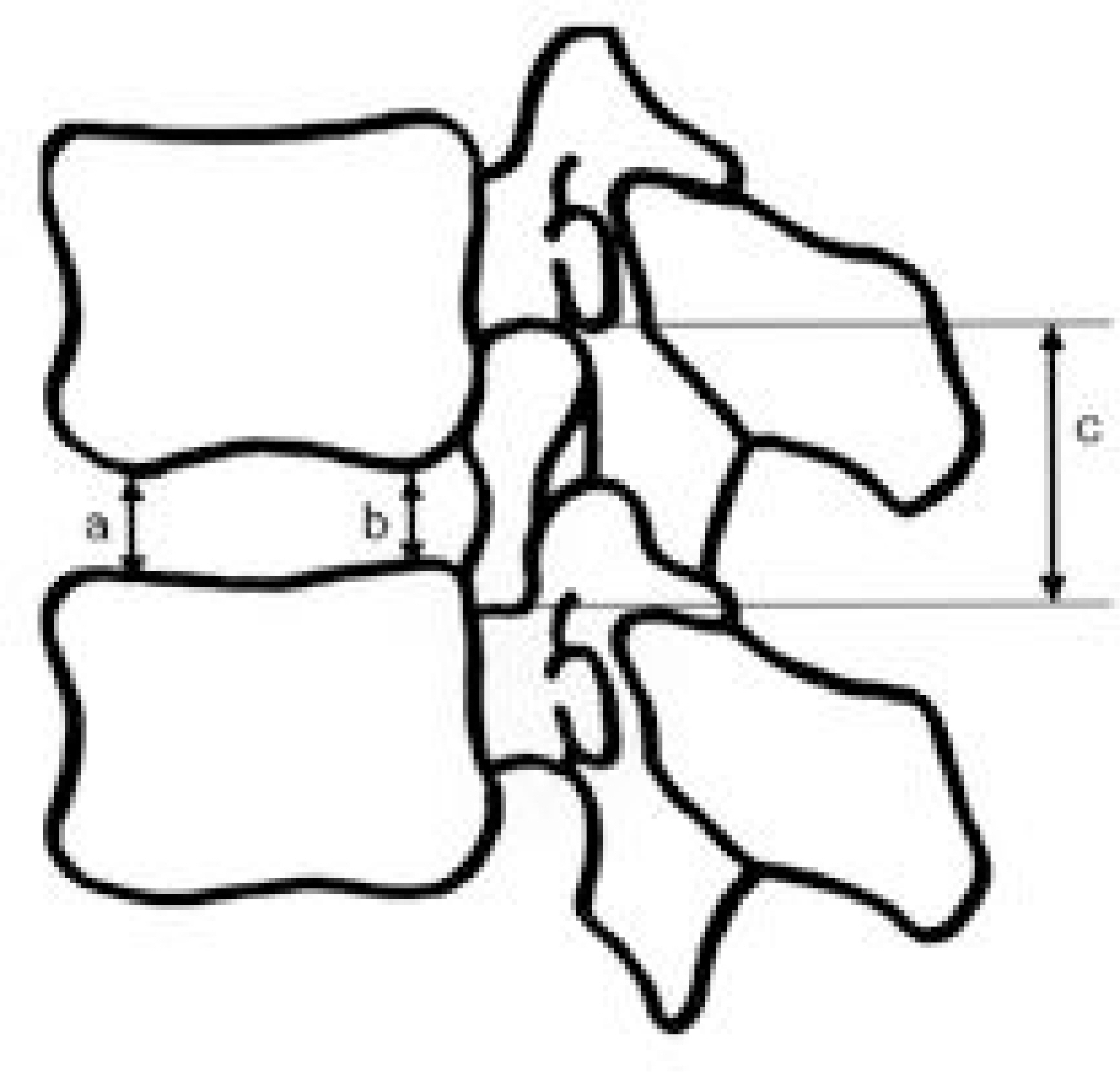
Fig. 2. Diagram showing the measurements made in the discs and neural foramens. (a) anterior disc height, (b) posterior disc height, (c) height of neural foramen
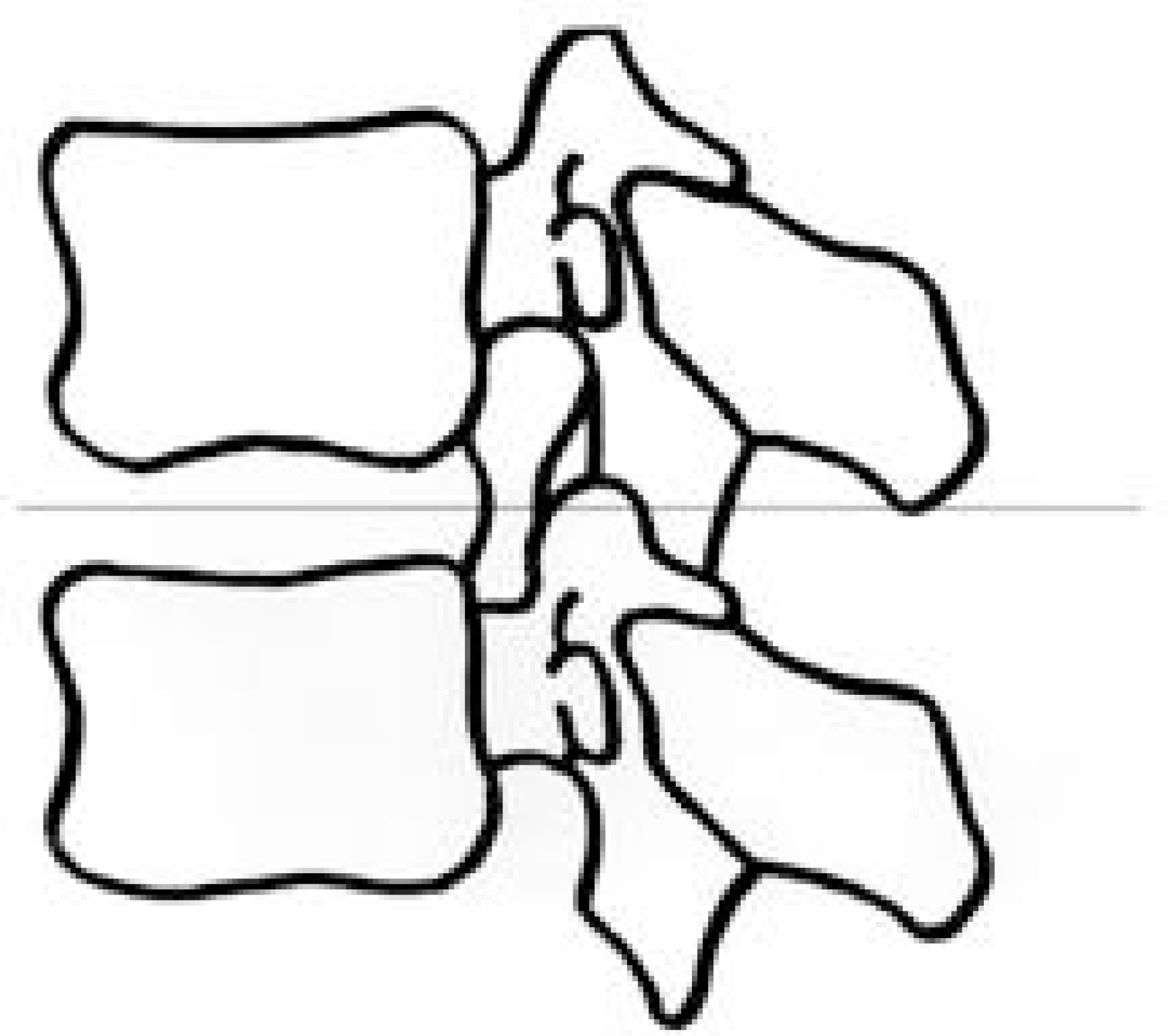
Fig. 3. CT measurement were done via axial image at the level of midportion of the disc on sagittal CT cut

Fig. 4. Diagram showing the measurements made in the axial image at the level of the midportion of the disc (a) midsagittal diameter of dural sac, (b) lateral diameter of dural sac, (c) area of dural sac, (d) diameter of lateral recess of neural canal

Fig. 5. A 34-year-old woman with spinal stenosis on L4-5. (A) Left side sagittal reconstruction image on preoperative CT scans. (B) Left side sagittal reconstruction image of seven-month postoperative CT scan shows marked increase of the anterior disc height, the posterior disc height and the height of neural foramen.

Fig. 6. A 34-year-old woman with spinal stenosis on L4-5. (A) Axial image of level of the midporion of the disc level on preoperative CT scan shows 6.60 mm in midsagittal diameter of dural sac, 8.89 mm in lateral diameter of dural sac, 65.96 mm in area of dural sac and diameter of lateral recess (right:3.41 mm, left:2.89 mm). (B) Axial image of level of the midporion of the disc level on eight-month postoperative CT scan shows 7.73 mm in midsagittal diameter of dural sac, 9.11 mm in lateral diameter of dural sac, 76.14 mm in area of dural sac and diameter of lateral recess (right: 3.87 mm, left: 3.85 mm).
Reference
-
1). Kirkaldy-Willis WH, McIVor G. Lumbar spinal steno -sis-editorial comment. Clin Orthop. 1976; 115:2–3.2). Vernon-Roberts B, Pirie C. Degenerative change in the intervertebral discs of the lumbar spine and their sequelae. Rheumatology and Rehabilitation. 1977; 16:13–21.3). Chen D, Fay LA, Lok F, Yuan P, Edwards WT, Yuan HA. Increasing neuroforaminal volume by anterior interbody distraction in degenerative lumbar spine. Spine. 1995; 20:74–79.
Article4). Van Akkerveeken PF. Lateral stenosis of the lumbar spine. Ph.D.thesis. University of Utrecht, Netherlands. 1989.5). Lee CK, Rauschning W, Glenn W. Lateral lumbar spinal canal stenosis. Classification, pathologic anatomy and surgical decompression. Spine. 1988; 13:313–321.
Article6). Edwards WC, LaRocca SH. The developmental segmental sagittal diameter in combined cervical and lumbar spondylosis. Spine. 1985; 10(1):42–54.
Article7). Ullrich CG, Binet EF, Sanecki MG, Kieffer SA. Quantitative assessment of the lumbar spinal canal by computed tomography. Radiology. 1980; 134:137–144.
Article8). Ciric I, Michael MA, Tarkington JA, Vick NA. The lateral recess syndrome. J Neurosurg. 1980; 53:433–439.
Article9). Shiradol O, Zdeblick TA, McAfee PC, Warden AK. Biomechanical evaluation of methods of posterior stabilization of the spine and posterior lumbar interbody arthrodesis for lumbosacral isthmic spondylolisthesis: A calf-spine model, J Bone Joint Surg[Am]. 1991; 73:518–526.10). Kirkaldy-Willis WH. The relationship of structural pathology to the nerve root. Spine. 1984; 9(1):49–52.
Article11). An HS, Glover JM. Lumbar spinal stenosis: Historical perspective, classification, and pathoanatomy. Semin Spine Surg. 1994. 67–77.12). Capener N. Spondylolithesis. Brit. J Surg. 1932; 19:374–380.13). Lane JD, Moore ES. Transperitoenal approach to the intervertebral disc in the lumbar area. Ann. Surg. 1948; 127:537–542.14). Harmon PH. Anterior excision and vertebral body fusion operation for intervertebral disc syndromes of the lower lumbar spine: Three to five-year results in 244 cases. Clin Orthop. 1963; 26:107–118.15). Goldner JL, Urbaniak JR, McCollumn DE. Ant erior disc excision and interbody spinal fusion for chronic low back pain. Orthop. Clin. North. Am. 1971; 2:543–552.16). Sacks S. Anterior interbody fusion of the lumbar spine. J Bone Joint Surg. 1965; 47-B:211–219.
Article17). Inufusa A. The Ideal Amount of Lumbar Foraminal Distraction for pedicle Screw Instrumentation. Spine. 1996; 21(19):2218–2223.
Article18). Inoue S, Watanabe T, Goto S, Tanahashi K, Takata K, Sho E. Degenerative spondylolisthesis: Pathophysiology and results of anterior inter body. Clin Orthop. 1988; 227:90–102.19). Inoue S, Watanabe T, Hirose A, et al. Anterior Discec -tomy and interbody fusion for lumbar disc herniation. Clin Orthop. 1984; 183:22–33.20). Kim NH, Kim HK, Suh JS. A computed tomographic analysis of changes in the spinal canal after anterior lumbar interbody fusion. Clin Orthop. 1993; 286:180–191.
Article21). Schlegel JD. The role of distraction in improving the spcace available in the lumbar stenotic canal and foramen Spine. 1994; 19(18):2041–2047.22). Jeon CH, Kim YC, Jung NS. Height changes of intervertebral disc and neural foramen after anterior lumbar interbody fusion in the lumbar spine. J Kor Spine Surg. 2003; 10(3):226–232.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Height Changes of Intervertebral Disc and Neural Foramen after Anterior Lumbar Interbody Fusion in the Lumbar Spine
- The Comparison of Changes in the Dimensions of the Intervertebral Disc and Neural Foramen between Anterior Lumbar Interbody Fusion and Posterolateral Fusion in the Lumbar Spine
- The Changes of Sagittal Alignment after Anterior Interbody Fusion with Posterior Fixation in Spondylolisthesis of the Lumbar Spine
- Letter: Comparison of Posterior Lumbar Interbody Fusion and Posterolateral Lumbar Fusion in Monosegmental Vacuum Phenomenon within an Intervertebral Disc
- The Changes in the Dimensions of Neural Foramen After Anterior Interbody Fusion in the Spondylolisthesis
