Korean J Obstet Gynecol.
2012 Apr;55(4):225-229. 10.5468/KJOG.2012.55.4.225.
Controversies surrounding type III radical abdominal hysterectomy and its procedure using new instruments
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Kurume University School of Medicine, Kurume, Japan. kimi@med.kurume-u.ac.jp
- KMID: 1992617
- DOI: http://doi.org/10.5468/KJOG.2012.55.4.225
Abstract
- Type III radical abdominal hysterectomy (RAH) is standard care for early stage cervical cancer. For the past few decades, there has been a remarkable shift from surgery to radiation, in the treatment choice for stage 1b2 and 2b cervical cancer in Japan. It is still controversial, however because some of those cases recommended RAH as a suitable treatment strategy. About 8% to 10% of RAH are abandoned because of tumor status. Recent preoperative screening cannot always detect them preoperatively. Various kinds of new surgical instruments, such as bipolar scissors and the electro vessel sealing system LigaSure have contributed to reducing the operation time and blood loss, in performing RAH. Furthermore, various kinds of devices are on the market. Surgeons should choose suitable instruments depending on the state of the disease and the patient.
Keyword
MeSH Terms
Figure
-
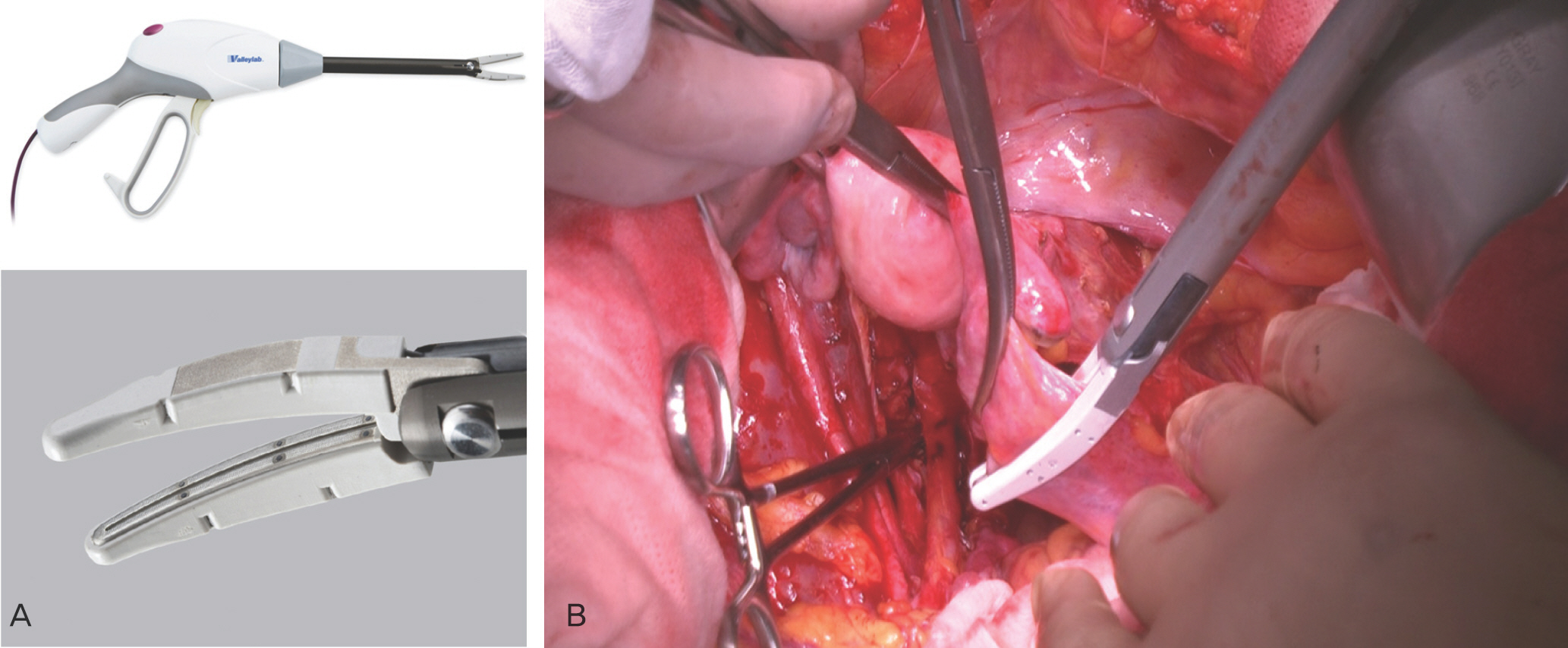
Fig. 1. LigaSure Impact. (A) LigaSure Impact has light angled jaw and scissors, useful for large vessls and pelvic floors. (B) Suspensorium ovary is clamped by LigaSure Impact.
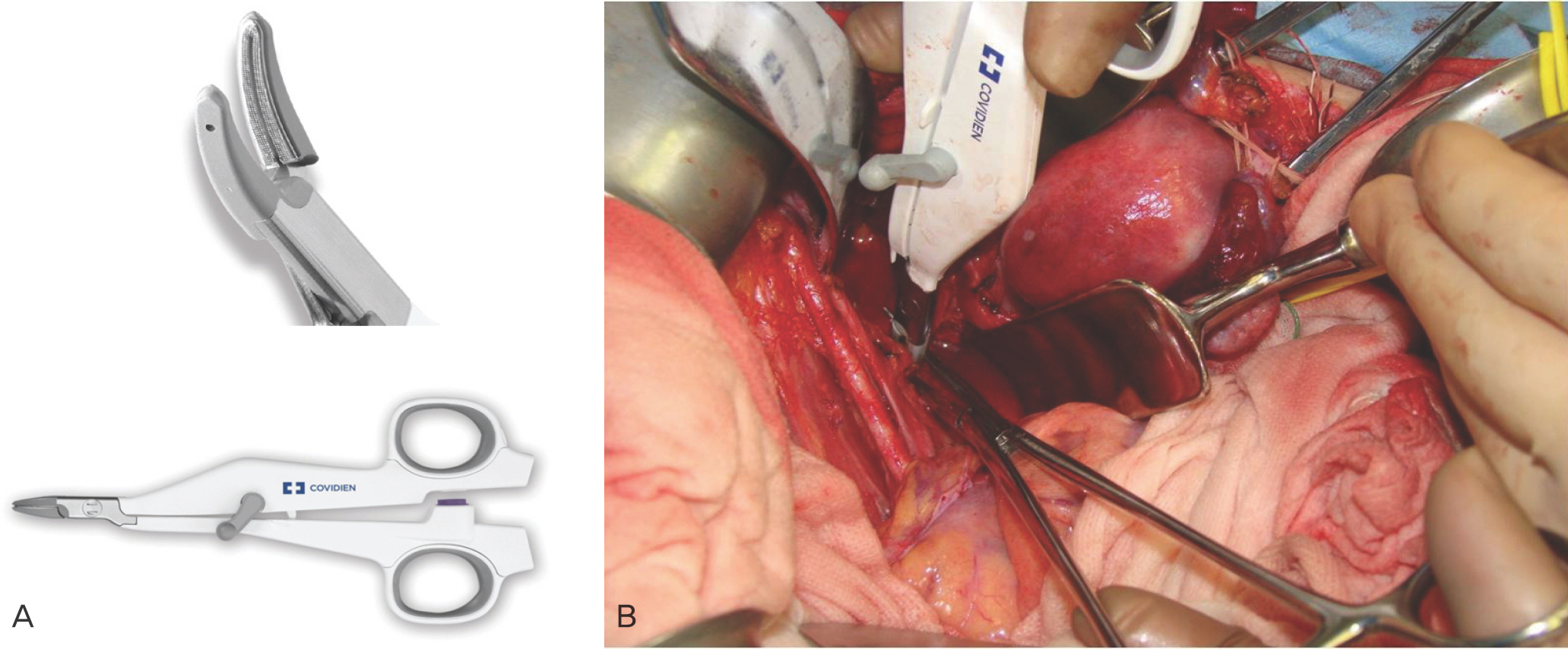
Fig. 2. LigaSure Small Jaw. (A) LigaSure Small Jaw has similar function with LigaSure Impact, also it has suitable size for narrow pelvic space. (B) Transection of cardinal ligament by LigaSure Small Jaw.
Reference
-
References
1. Piver MS, Rutledge F, Smith JP. Five classes of extended hysterectomy for women with cervical cancer. Obstet Gynecol. 1974; 44:265–72.
Article2. Whitney CW, Sause W, Bundy BN, Malfetano JH, Hannigan EV, Fowler WC Jr, et al. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stage IIB-IVA carcinoma of the cervix with negative paraaortic lymph nodes: a Gynecologic Oncology Group and Southwest Oncology Group study. J Clin Oncol. 1999; 17:1339–48.
Article3. Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, Stevens RE, et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and paraaortic radiation for high-risk cervical cancer. N Engl J Med. 1999; 340:1137–43.
Article4. Rose PG, Bundy BN, Watkins EB, Thigpen JT, Deppe G, Maiman MA, et al. Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. N Engl J Med. 1999; 340:1144–53.
Article5. Japanese Society of Gynecologist and Obstetrician tumor committee report. Acta Obstet Gynaecol Jpn. 2002; 54:1527–72.6. Landoni F, Maneo A, Colombo A, Placa F, Milani R, Perego P, et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet. 1997; 350:535–40.
Article7. Yamashita H, Nakagawa K, Tago M, Shiraishi K, Nakamura N, Ohtomo K, et al. Comparison between conventional surgery and radiotherapy for FIGO stage I-II cervical carcinoma: a retrospective Japanese study. Gynecol Oncol. 2005; 97:834–9.
Article8. Zivanovic O, Alektiar KM, Sonoda Y, Zhou Q, Iasonos A, Tew WP, et al. Treatment patterns of FIGO Stage IB2 cervical cancer: a single-institution experience of radical hysterectomy with individualized postoperative therapy and definitive radiation therapy. Gynecol Oncol. 2008; 111:265–70.
Article9. Tattersall MH, Lorvidhaya V, Vootiprux V, Cheirsilpa A, Wong F, Azhar T, et al. Randomized trial of epirubicin and cisplatin chemotherapy followed by pelvic radiation in locally advanced cervical cancer. Cervical Cancer Study Group of the Asian Oceanian Clinical Oncology Association. J Clin Oncol. 1995; 13:444–51.
Article10. Japanese Society of Gynecologist and Obstetrician tumor committee report. Acta Obstet Gynaecol Jpn. 2011; 63:1055–96.11. Whitney CW, Stehman FB. The abandoned radical hysterectomy: a Gynecologic Oncology Group Study. Gynecol Oncol. 2000; 79:350–6.
Article12. Richard SD, Krivak TC, Castleberry A, Beriwal S, Kelley JL 3rd, Edwards RP, et al. Survival for stage IB cervical cancer with positive lymph node involvement: a comparison of completed vs. abandoned radical hysterectomy. Gynecol Oncol. 2008; 109:43–8.
Article13. Lee MJ, Yun MJ, Park MS, Cha SH, Kim MJ, Lee JD, et al. Paraaortic lymph node metastasis in patients with intraabdominal malignancies: CT vs PET. World J Gastroenterol. 2009; 15:4434–8.
Article14. Boughanim M, Leboulleux S, Rey A, Pham CT, Zafrani Y, Duvil-lard P, et al. Histologic results of paraaortic lymphadenectomy in patients treated for stage IB2/II cervical cancer with negative [18F]fluorodeoxyglucose positron emission tomography scans in the paraaortic area. J Clin Oncol. 2008; 26:2558–61.
Article15. Silva-Filho AL, Rodrigues AM, Vale de Castro Monteiro M, da Rosa DG, Pereira e Silva YM, Werneck RA, et al. Randomized study of bipolar vessel sealing system versus conventional suture ligature for vaginal hysterectomy. Eur J Obstet Gynecol Reprod Biol. 2009; 146:200–3.
Article16. Kyo S, Mizumoto Y, Takakura M, Hashimoto M, Mori N, Ikoma T, et al. Experience and efficacy of a bipolar vessel sealing system for radical abdominal hysterectomy. Int J Gynecol Cancer. 2009; 19:1658–61.
Article17. Tamussino K, Afschar P, Reuss J, Perschler M, Ralph G, Winter R. Electrosurgical bipolar vessel sealing for radical abdominal hysterectomy. Gynecol Oncol. 2005; 96:320–2.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The twenty-first century role of Piver-Rutledge type III radical hysterectomy and FIGO stage IA, IB1, and IB2 cervical cancer in the era of robotic surgery: a personal perspective
- Vaginal evisceration after radical hysterectomy and adjuvant radiation
- Cost-effectiveness analysis of simple hysterectomy compared to radical hysterectomy for early cervical cancer: analysis from the GCIG/CCTG CX.5/SHAPE trial
- Improved bladder function in radical hysterectomy without worsening oncologic outcome: resection of the posterior layer of the vesicouterine ligament with the procedure limited to the vesical veins
- Comparative Effectiveness of Abdominal versus Laparoscopic Radical Hysterectomy for Cervical Cancer in the Postdissemination Era
