A Case of Adenocarcinoma Presenting a Solitary Pulmonary Nodule that Grows Slowly Over 10 Years
- Affiliations
-
- 1Department of Internal Medicine, Soonchunhyang University College of Medicine, Cheonan, Korea. cjssch@hanmail.net
- 2Department of Pathology, Soonchunhyang University College of Medicine, Cheonan, Korea.
- KMID: 1970185
- DOI: http://doi.org/10.4046/trd.2008.64.4.318
Abstract
- It is difficult to distinguish a lung cancer from a pulmonary tuberculoma or other benign nodule. It is even more difficult to identify the type of lesion if the mass shows no change in size or demonstrates slow growth. Only a pathological confirmation can possibly reveal the nature of the lesion. A 61-year-old-woman was referred for a solitary pulmonary nodule. The nodule showed no change in size for the first two years and continued to grow slowly. Pathological and immunological analyses were conducted for confirmation of the nodule. The nodule was identified as a well-differentiated primary pulmonary adenocarcinoma. An LULobectomy was performed, and the post surgical stage of the nodule was IIIA (T2N2M0). Even though there are few risk factors, there is still the possibility of a malignancy in cases of non-growing or slow growing solitary pulmonary nodules. Therefore, pathological confirmation is encouraged to obtain a firm diagnosis.
Figure
-
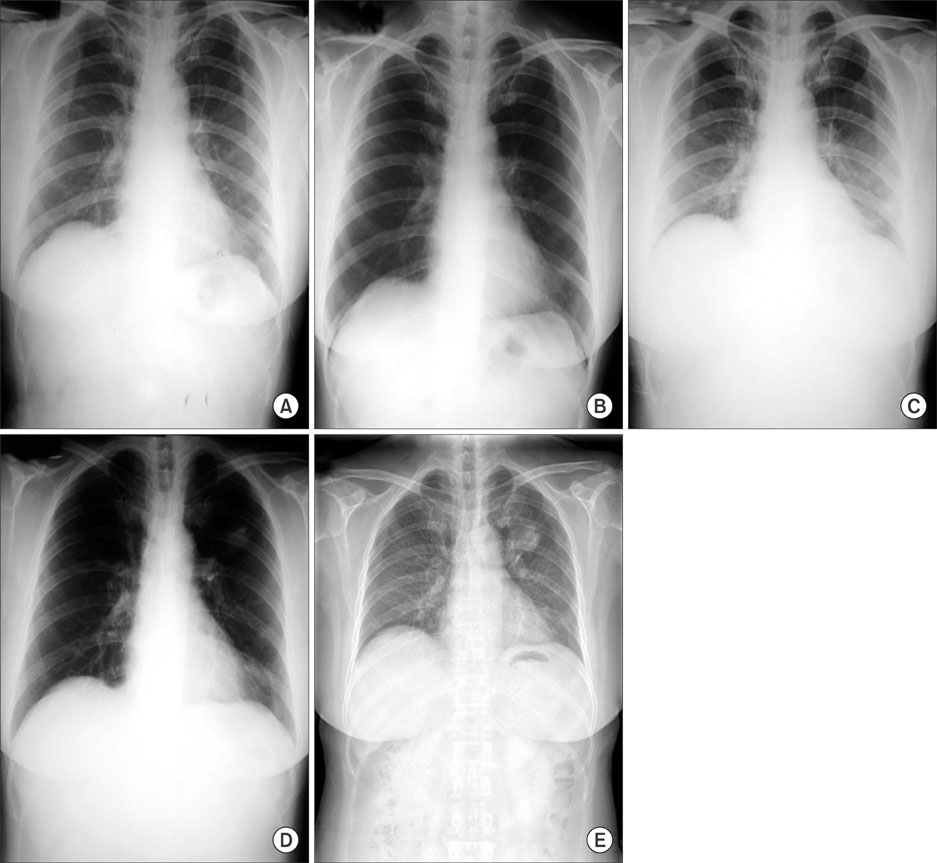
Figure 1 Serial chest PAs show solitary pulmonary masses in left upper lobe. The mass was approximately 1.6 cm in size in 1997 and 3.5 cm in 2006 by slow growing. September, 1997 (A), November, 1998 (B), October, 1999 (C), May, 2004 (D), April, 2006 (E).

Figure 2 Conventional chest CT scan reveals solitary 3.5 cm sized lung mass in left upper lobe without lynphadenopathy. The distal porton of the mass shows an atelectasis.
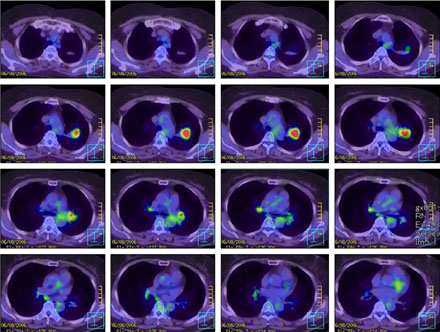
Figure 3 PET-CT scan reveals hypermetabolic activity in the left upper lobe mass measured 3.5 cm. The contralateral hilar, subcarinal and interlobar lymph nodes are considered as benign conditions with the calculated SUVs less than 2.5.
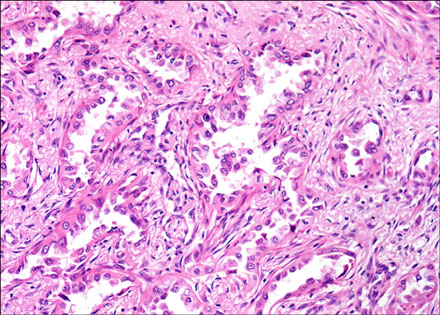
Figure 4 Microscopic finding shows a well differentiated adenocarcinoma (H&E stain, ×200).
Reference
-
1. Ryu NS, Kim SJ, Kim SK, Lee KD, Kim JH, Cho DI, et al. Clinical study on lung cancer associated with pulmonary tuberculosis. Tuberc Respir Dis. 1986. 33:35–42.2. Jung TH. Diagnosis of lung cancer. Tuberc Respir Dis. 1990. 37:337–347.3. Kho WJ, Kim CH, Jang SH, Lee JH, Yoo CG, Chung HS, et al. Diagnostic approach to the solitary pulmonary nodule: reappraisal of the traditional clinical parameters for differentiating malignant nodule from benign nodule. Tuberc Respir Dis. 1996. 43:500–518.4. Tan BB, Flaherty KR, Kazerooni EA, Iannettoni MD. The solitary pulmonary nodule. Chest. 2003. 123:89S–96S.5. Lillington GA. Management of solitary pulmonary nodules. Dis Mon. 1991. 37:271–318.6. Becker GL, Whitlock WL, Schaefer PS, Tenholder MF. The impact of thoracic computed tomography in clinically staged T1, N0, M0 chest lesions. Arch Intern Med. 1990. 150:557–559.7. Yoon BK, Kim EJ, Kim DI, Lee KH, Ryu JS, Kwak SM, et al. A case of adenocarcinoma presenting a solitary pulmonary nodule that showed no growth over 4 years. Tuberc Respir Dis. 2005. 59:326–329.8. Midthun DE, Swensen SJ, Jett JR. Approach to the solitary pulmonary nodule. Mayo Clin Proc. 1993. 68:378–385.9. Remy-Jardin M, Remy J, Giraud F, Marquette CH. Pulmonary nodules: detection with thick-section spiral CT versus conventional CT. Radiology. 1993. 187:513–520.10. Collins VP, Loeffler RK, Tivey H. Observations on growth rates of human tumors. Am J Roentgenol Radium Ther Nucl Med. 1956. 76:988–1000.11. Sung DW. Radiological findings of lung cancer: focus on atypical pattern. Tuberc Respir Dis. 2005. 58:554–561.12. Erasmus JJ, Connolly JE, McAdams HP, Roggli VL. Solitary pulmonary nodules: Part I. morphologic evaluation for differentiaton of benign and malignant lesions. Radiographics. 2000. 20:43–58.13. Yankelevitz DF, Henschke CI. Does 2-year stability imply that pulmonary nodules are benign? AJR Am J Roentgenol. 1997. 168:325–328.14. Woodring JH, Stelling CB. Adenocarcinoma of the lung: a tumor with a changing pleomorphic character. AJR Am J Roentgenol. 1983. 140:657–664.15. Hollings N, Shaw P. Diagnostic imaging of lung cancer. Eur Respir J. 2002. 19:722–742.16. Gupta NC, Maloof J, Gunel E. Probability of malignancy in solitary pulmonary nodules using fluorine-18-FDG and PET. J Nucl Med. 1996. 37:943–948.17. Kim WJ, Yim JJ, Yoo CG, Kim YW, Shim YS, Han SK. Diagnositic efficacy of FDG-PET in solitary pulmonary nodule. Tuberc Respir Dis. 1997. 44:1263–1270.18. Kim GS, Im SC, Go YC, Park GH, Ju JY, Jo GJ, et al. Utility of FDG-PET in solitary pulmonary nodules and the relationship between standardized uptake values of PET and serum glucose. Tuberc Respir Dis. 2003. 55:589–596.19. Ost D, Fein AM, Feinsilver SH. Clinical practice. The solitary pulmonary nodule. N Engl J Med. 2003. 348:2535–2542.20. MacMahon H, Austin JH, Gamsu G, Herold CJ, Jett JR, Naidich DP, et al. Guidelines for management of small pulmonary solitary nodules detected on CT scans: a statement from the Fleischner Society. Radiology. 2005. 237:395–400.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Adenocarcinoma Presenting a Solitary Pulmonary Nodule That Showed No Growth Over 4 Years
- Primary Intrapulmonary Thymoma Presenting as a Solitary Pulmonary Nodule
- Treatment of Sclerosing Hemangioma by Lobectomy : A case report
- Solitary Pulmonary Nodule
- Bronchioloalveolar Cell Carcinoma in Solitary Pulmonary Nodule(SPN) with Cavitary Lesion
