J Korean Orthop Assoc.
2007 Dec;42(6):828-831. 10.4055/jkoa.2007.42.6.828.
LumbarWedgeResectionOsteotomyforCongenitalScoliosis duetoaSacralMalformation: A CaseReport
- Affiliations
-
- 1Department of Orthopaedic Surgery, Halla General Hospital, Jeju, Korea. dominant0526@naver.com
- KMID: 1947792
- DOI: http://doi.org/10.4055/jkoa.2007.42.6.828
Abstract
- Congenital scoliosis due to a sacral malformation is quite rare. To the best of our knowledge, most wedge resection osteotomies have been performed to correct a kyphotic deformity in ankylosing spondylitis. However, there is no report of a trapezoidal lumbar wedge resection osteotomy of the vertebral body in the surgical treatment of congenital scoliosis due to a sacral malformation. This paper reports a 41-year-old female with a 25-year history of lower back and buttock pain combined with radiating pain to the lower extremities. The coronal imbalance was 3.8 cm and the scoliosis angle using the Cobb method was 22 degrees. A trapezoidal wedge resection osteotomy of the L5 body was performed, and the scoliosis was corrected. We detail this modification of a vertebral osteotomy technique and show that a fixed coronal deformity could be corrected effectively using this technique.
Keyword
MeSH Terms
Figure
-
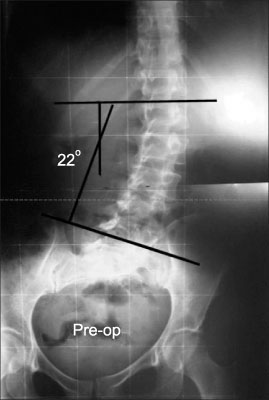
Fig. 1 Pre-operative anteroposterior standing radiograph reveals the malformation of the sacrum and pelvis, and 22 degrees of scoliosis angle between L1 and L5.
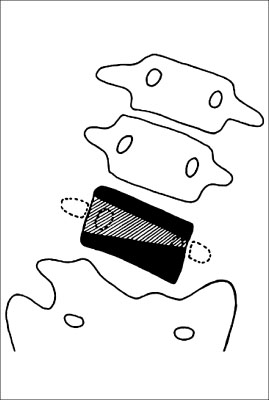
Fig. 2 The illustration of the pre-operative planning of the osteotomy. The hatched marks define the extent of the osteotomy.
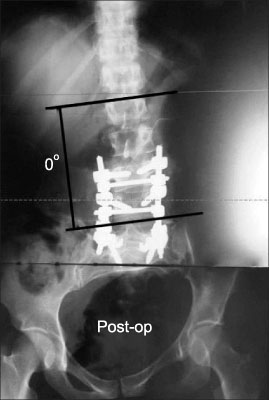
Fig. 3 Post-operative anteroposterior standing radiograph reveals the correction of the scoliosis angle between L1 and L5.
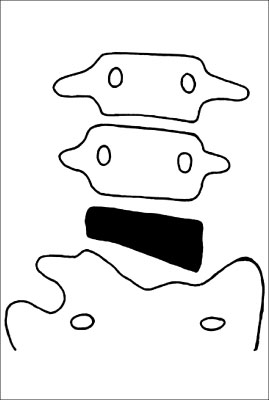
Fig. 4 The illustration of the postoperative status. The scoliosis was corrected with a trapezoidal wedge resection osteotomy of L5.
Reference
-
1. Boachie-Adjei O, Ferguson JA, Pigeon RG, Peskin MR. Transpedicular lumbar wedge resection osteotomy for fixed sagittal imbalance: surgery technique and early results. Spine. 2006. 31:485–492.2. Bradford DS, Tribus CB. Vertebral column resection for the treatment of rigid coronal decompensation. Spine. 1997. 22:1590–1599.
Article3. Bridwell KH, Lewis SJ, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. J Bone Joint Surg Am. 2003. 85:454–463.
Article4. Cho KJ, Bridwell KH, Lenke LG, Berra A, Baldus C. Comparison of Smith-Petersen versus pedicle subtraction osteotomy for the correction of fixed sagittal imbalance. Spine. 2005. 30:2030–2037.
Article5. Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine. 2002. 27:612–618.
Article6. Suk SI, Chung ER, Lee SM, Lee JH, Kim SS, Kim JH. Posterior vertebral column resection in fixed lumbosacral deformity. Spine. 2005. 30:E703–E710.
Article7. Suk SI, Kim JH, Kim WJ, Lee SM, Chung ER, Nah KH. Posterior vertebral column resection for severe spinal deformities. Spine. 2002. 27:2374–2382.
Article8. Thomasen E. Vertebral osteotomy for correction of kyphosis in ankylosing spondylitis. Clin Orthop Relat Res. 1985. 194:142–152.
Article9. van Royen BJ, Slot GH. Closing-wedge posterior osteotomy for ankylosing spondylitis. Partial corporectomy and transpedicular fixation in 22 cases. J Bone Joint Surg Br. 1995. 77:117–121.
Article10. Winter RB, Moe JH, Eilers VE. Congenital scoliosis. A study of 234 patients treated and untreated. J Bone Joint Surg Am. 1968. 50:1–47.
Article
