Percutaneous Closure of an Iatrogenic Ventricular Septal Defect Following Concomitant Septal Myectomy at the Time of Aortic Valve Replacement
- Affiliations
-
- 1Department of Internal Medicine, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea.
- 2Division of Thoracic and Cardiovascular Surgery, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea. jinho@eulji.ac.kr
- KMID: 1859242
- DOI: http://doi.org/10.4070/kcj.2014.44.1.45
Abstract
- A 77-year-old female patient underwent aortic valve replacement (AVR) with concomitant septal myectomy and tricuspid annuloplasty. Her symptoms did not improve after a successful operation. Echocardiogram demonstrated the presence of an iatrogenic ventricular septal defect (VSD). It was muscular in location and not the usual AVR with membraneous type of VSD, suggesting a complication from the myectomy. Percutaneous closure of the VSD remained the only feasible option due to her poor overall medical status. A 14-mm Amplazter VSD occluder was deployed successfully, by means of the trans-septal technique. She has improved very well postoperatively.
MeSH Terms
Figure
-

Fig. 1 Iatrogenic VSD assessment by echocardiography. A: parasternal long-axis view shows a muscular VSD (arrow), suggesting of a complication by myectomy, not AVR in which it is usually present with membraneous type of VSD. B: color Doppler imaging depicts a high-velocity jet between the left ventricle and right ventricle. C: the velocity and peak pressure gradient across the defect are measured at 4.78 m/s and 91.33 mm Hg, respectively. VSD: ventricular septal defect, AVR: aortic valve replacement, RV: right atrium, LV: left ventricle, Ao: aorta.
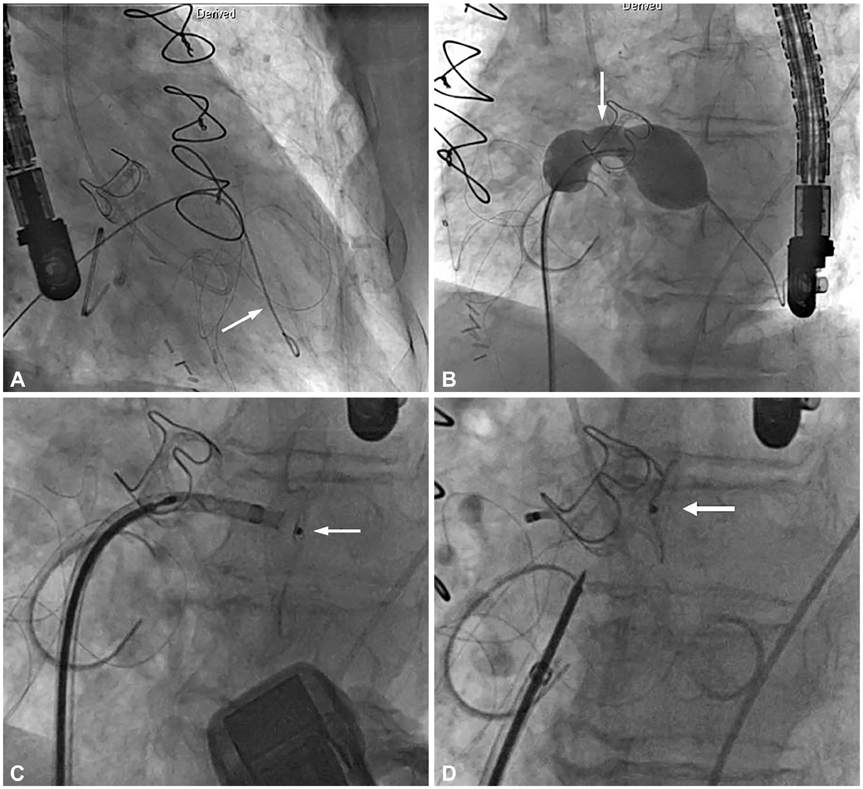
Fig. 2 Placement of Percutaneous Amplatzer Muscular ventricular septal defect (VSD) occluder. A: a 0.035 inch extra-stiff guide wire (arrow) is advanced from the femoral vein through the defect, and into the left ventricle (LV) apex. B: the diameter of Amplazter VSD occluder is measured using an Amplazter sizing balloon II (arrow). C: the LV disc of the Amplazter VSD occluder (arrow) is deployed first in the LV. D: it has released the right ventricle (RV) disc of the device (arrow) in the RV by rotating the delivery cable in a counterclockwise direction.
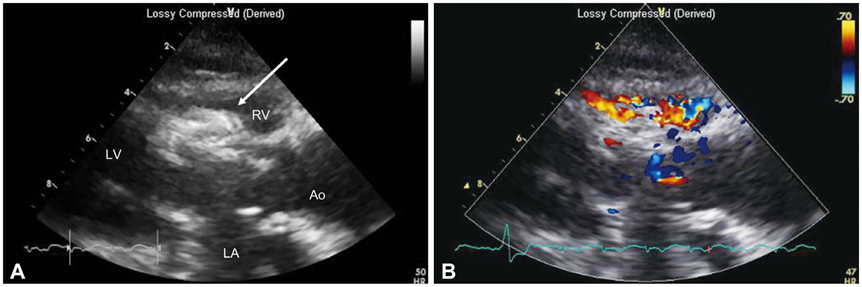
Fig. 3 Post-procedural echocardiography. A: parasternal long axis view shows the appropriate positioning of the Amplazter ventricular septal defect occluder. The device is seen as a dense crescent-like structure (arrow), at the left side of the interventricular septum. The left ventricular outflow tract is not obstructed. B: color Doppler imaging shows near-elimination of the left to right shunt after device delivery. RV: right ventricle, LV: left ventricle, LA: left atrium, Ao: aorta.
Reference
-
1. Panza JA, Maron BJ. Valvular aortic stenosis and asymmetric septal hypertrophy: diagnostic considerations and clinical and therapeutic implications. Eur Heart J. 1988; 9:Suppl E. 71–76.2. Kayalar N, Schaff HV, Daly RC, Dearani JA, Park SJ. Concomitant septal myectomy at the time of aortic valve replacement for severe aortic stenosis. Ann Thorac Surg. 2010; 89:459–464.3. Hess OM, Schneider J, Turina M, Carroll JD, Rothlin M, Krayenbuehl HP. Asymmetric septal hypertrophy in patients with aortic stenosis: an adaptive mechanism or a coexistence of hypertrophic cardiomyopathy? J Am Coll Cardiol. 1983; 1:783–789.4. Carminati M, Butera G, Chessa M, et al. Transcatheter closure of congenital ventricular septal defects: results of the European Registry. Eur Heart J. 2007; 28:2361–2368.5. Holzer R, de Giovanni J, Walsh KP, et al. Transcatheter closure of perimembranous ventricular septal defects using the amplatzer membranous VSD occluder: immediate and midterm results of an international registry. Catheter Cardiovasc Interv. 2006; 68:620–628.6. Minakata K, Dearani JA, O'Leary PW, Danielson GK. Septal myectomy for obstructive hypertrophic cardiomyopathy in pediatric patients: early and late results. Ann Thorac Surg. 2005; 80:1424–1429. discussion 1429-30.7. Valeti US, Nishimura RA, Holmes DR, et al. Comparison of surgical septal myectomy and alcohol septal ablation with cardiac magnetic resonance imaging in patients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol. 2007; 49:350–357.8. Kilicgedik A, Karabay CY, Aung SM, et al. A successful percutaneous closure of ventricular septal defect following septal myectomy in patients with hypertrophic obstructive cardiomyopathy. Perfusion. 2012; 27:253–255.9. Spies C, Ujivari F, Schraeder R. Transcatheter closure of a ventricular septal defect following myectomy for hypertrophic obstructive cardiomyopathy. Cardiology. 2009; 112:31–34.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report of Ventricular Septal Defect and Aortic Valve Insufficiency Occurred in Siblings
- Mitral Valve Replacement in Children and Adolescence using Bioprosthetic Valve or Prosthetic Valve
- Pulmonary Thromboembolism and Infarction Caused by Right-Sided Infective Endocarditis in a Patient with Ventricular Septal Defect
- Postoperative Evaluation for Ventricular Septal Defect Associated with Aortic Valvular Prolapse
- Tips for Successful Septal Myectomy in Patients with Hypertrophic Cardiomyopathy
