Pulmonary Cryptococcosis That Mimicked Rheumatoid Nodule in Rheumatoid Arthritis Lesion
- Affiliations
-
- 1Department of Internal Medicine, National Medical Center, Seoul, Korea. inajeong@gmail.com
- 2Department of Pathology, National Medical Center, Seoul, Korea.
- 3Department of Thoracic and Cardiovascular Surgery, National Medical Center, Seoul, Korea.
- KMID: 1842995
- DOI: http://doi.org/10.4046/trd.2014.77.6.266
Abstract
- Recently, the incidence of pulmonary cryptococcosis is gradually increasing in rheumatoid arthritis (RA) patients. Pulmonary rheumatoid nodules (PRN) are rare manifestations of RA. Eighteen months ago, a 65-year old woman was admitted to hospital due to multiple nodules (2.5x2.1x2 cm) with cavitations in the right lower lobe. She was diagnosed with RA three year ago. She had been taking methotrexate, leflunomide, and triamcinolone. A video-assisted thoracoscopic surgery biopsy was performed and PRN was diagnosed. However, a newly growing huge opacity with cavitation was detected in the same site. Pulmonary cryptococcal infection was diagnosed through a transthoracic computed tomograpy guided needle biopsy. Cryptococcus antigen was detected in serum but not in cerebrospinal fluid. The patient was treated with oral fluconazole which resulted clinical improvement and regression of the nodule on a series of radiography. Herein, we report the case of pulmonary cryptococcosis occurring in the same location as that of the PRN.
MeSH Terms
Figure
-

Figure 1 Radiologic findings. (A) Multifocal area of small nodules with cavitation in the right lower lung fields at 21 months prior to admission. (B) Postoperative sequalae was noted after 11 months of video-assisted thoracoscopic surgery biopsy. (C) Huge opacity with cavitation growing in the right lower lung fields at the time of admission. (D) Chest posteroanterior view and computed tomographic image showing a decrease in the size of the consolidative huge opacity after treatment with oral fluconazole at 400 mg daily for 4 months.
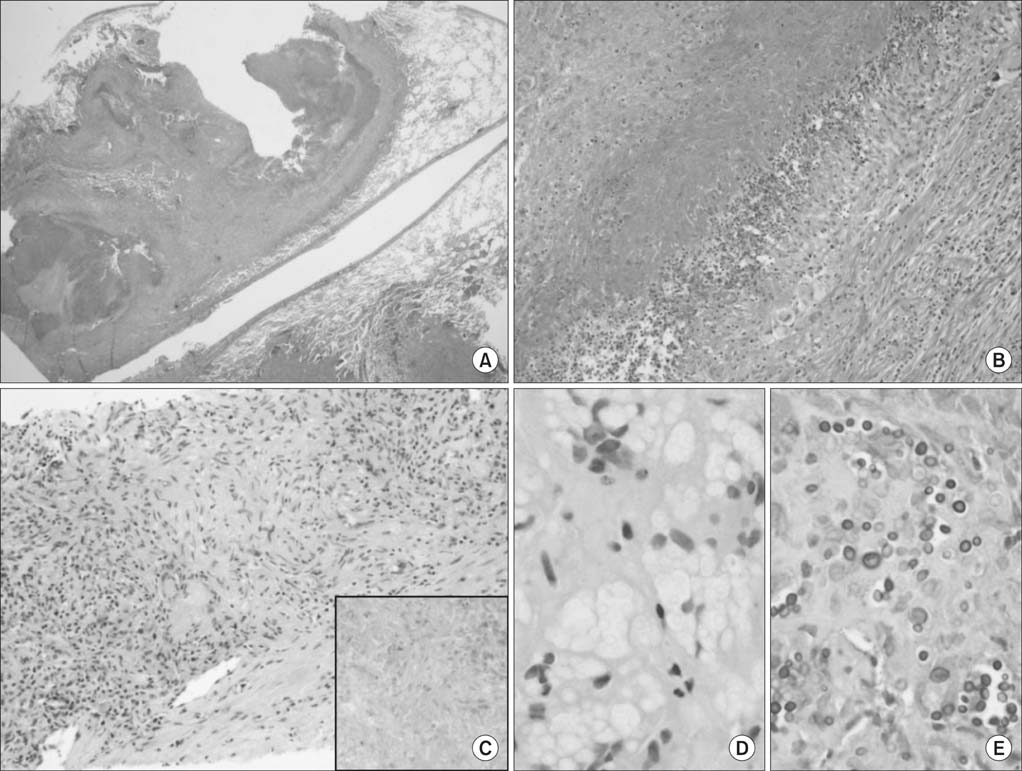
Figure 2 Histological features of the first (A and B) and newly developed pulmonary lesions (C-E). (A) Low magnification of the first lesion located in the subpleural lung region showing necrotising granulomas. (B) The granulomas consisting of central necrosis (left upper side) surrounded by palisading epithelioid histiocytes, multinucleated giant cells, and chronic inflammation (right lower side). No definite histological features suggestive of vasculitides were observed. Special stainings including Ziehl-Neelsen, Grocott-Gomori methenamine silver, and periodic acid-Schiff staining showed no acid-fast bacilli or fungi (figures not shown). These features combined with the clinical findings suggest a diagnosis of necrobiotic nodules caused by rheumatoid arthritis. (C) The newly developed lesion showing granulomas containing epithelioid histiocytes, multinucleated giant cells, and chronic inflammation. Some of the epithelioid histiocytes had bubbly cytoplasms. The lesion was accompanied by a necrotic fragment (inset). (D) At higher magnification, the typical round, pale intracellular organisms with a clear halo could be seen in the viable epithelioid histiocytes. (E) The periodic acid-Schiff stain is positive for round yeasts. These features are compatible with a diagnosis of cryptococcosis (A, H&E stain, ×12.5; B, H&E stain, ×100; C, H&E stain, ×200; D, H&E stain, ×400; E, periodic acid-Schiff stain, ×400).
Reference
-
1. Anaya JM, Diethelm L, Ortiz LA, Gutierrez M, Citera G, Welsh RA, et al. Pulmonary involvement in rheumatoid arthritis. Semin Arthritis Rheum. 1995; 24:242–254.2. Gomez Herrero H, Arraiza Sarasa M, Rubio Marco I, Garcia de Eulate Martin-Moro I. Pulmonary rheumatoid nodules: presentation, methods, diagnosis and progression in reference to 5 cases. Reumatol Clin. 2012; 8:212–215.3. Aberg JA, Mundy LM, Powderly WG. Pulmonary cryptococcosis in patients without HIV infection. Chest. 1999; 115:734–740.4. Kim YS, Lee IH, Kim HS, Jin SS, Lee JH, Kim SK, et al. Pulmonary cryptococcosis mimicking primary lung cancer with multiple lung metastases. Tuberc Respir Dis. 2012; 73:182–186.5. Nunez M, Peacock JE Jr, Chin R Jr. Pulmonary cryptococcosis in the immunocompetent host. Therapy with oral fluconazole: a report of four cases and a review of the literature. Chest. 2000; 118:527–534.6. Caporali R, Caprioli M, Bobbio-Pallavicini F, Montecucco C. DMARDS and infections in rheumatoid arthritis. Autoimmun Rev. 2008; 8:139–143.7. Hage CA, Wood KL, Winer-Muram HT, Wilson SJ, Sarosi G, Knox KS. Pulmonary cryptococcosis after initiation of anti-tumor necrosis factor-alpha therapy. Chest. 2003; 124:2395–2397.8. Yoo HG, Yu HM, Jun JB, Jeon HS, Yoo WH. Risk factors of severe infections in patients with rheumatoid arthritis treated with leflunomide. Mod Rheumatol. 2013; 23:709–715.9. Yanagawa N, Sakai F, Takemura T, Ishikawa S, Takaki Y, Hishima T, et al. Pulmonary cryptococcosis in rheumatoid arthritis (RA) patients: comparison of imaging characteristics among RA, acquired immunodeficiency syndrome, and immunocompetent patients. Eur J Radiol. 2013; 82:2035–2042.10. Morita Y, Katoh S, Watanabe H, Harada H, Uno E, Satoh M, et al. Rheumatoid nodules of the lung in a patient with palindromic rheumatism. Intern Med. 1992; 31:951–954.11. Song KD, Lee KS, Chung MP, Kwon OJ, Kim TS, Yi CA, et al. Pulmonary cryptococcosis: imaging findings in 23 non-AIDS patients. Korean J Radiol. 2010; 11:407–416.12. Adelman HM, Dupont EL, Flannery MT, Wallach PM. Case report: recurrent pneumothorax in a patient with rheumatoid arthritis. Am J Med Sci. 1994; 308:171–172.13. Cavazza A, Paci M, Turrini E, Dallari R, Rossi G. Fungus colonisation of pulmonary rheumatoid nodule. J Clin Pathol. 2003; 56:636–637.14. Winne L, Praet M, Brusselle G, Veys E, Mielants H. Bilateral spontaneous pneumothorax in a patient with pulmonary rheumatoid nodules, secondary infected by Aspergillus. Clin Rheumatol. 2007; 26:1180–1182.15. Scully RE, Mark EJ, McNeely WF, Ebeling SH, Phillips LD. Case records of the Massachusetts General Hospital Weekly clinicopathological exercises. Case 20-1997. A 74-year-old man with progressive cough, dyspnea, and pleural thickening. N Engl J Med. 1997; 336:1895–1903.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Cryptococcosis in Rheumatoid Arthritis Patient Treated With Leflunomide
- A Case of Rheumatoid Nodule in a Systemic Lupus Erythematosus Patient
- Clinical significance of rheumatoid factor in juvenile rheumatoid arthritis
- A Case of Pulmonary Cryptococcosis in a Patient with Rheumatoid Arthritis
- Development of Rheumatoid Nodules after Anti-Tumor Necrosis Factor-α Treatment with Adalimumab for Rheumatoid Arthritis
