Spinopelvic Fixation
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. bschang@snu.ac.kr
- KMID: 1819814
- DOI: http://doi.org/10.4184/jkss.2009.16.4.304
Abstract
- Lumbosacral fixation or spinopelvic fixation is frequently required for the surgical treatment of neuromuscular scoliosis and degenerative lesions, trauma and tumor in the lumbosacral vertebrae. However, the establishment of stable fixation with these procedures is difficult due to the anatomic characteristics of the sacrum and this is even more problematic for the cases with long segmental fixation, severe instability and bone defects. Although the emergence of pedicle screws makes spinal fixation easier and more rigid, S1 pedicle screws alone do not provide enough stability for lumbosacral fixation. For the purposes of reinforcing lumbosacral fixation, procedures using rods or screws can be used: the procedures using rods include the Galveston method, the McCarthy S-rod and the Jackson intrasacral rod, and the procedures using screws include sacral alar screws, transdiscal screws and iliac screws. The purpose of this study was to ascertain the proper fixation methods, according to each indication, for spinopelvic fixation and we analyzed the advantages and drawbacks of each fixation method. In addition, the fixation method of iliac screws, which has recently become more popular, is presented in detail to enhance the availability and reduce the complication of this technique.
MeSH Terms
Figure
-
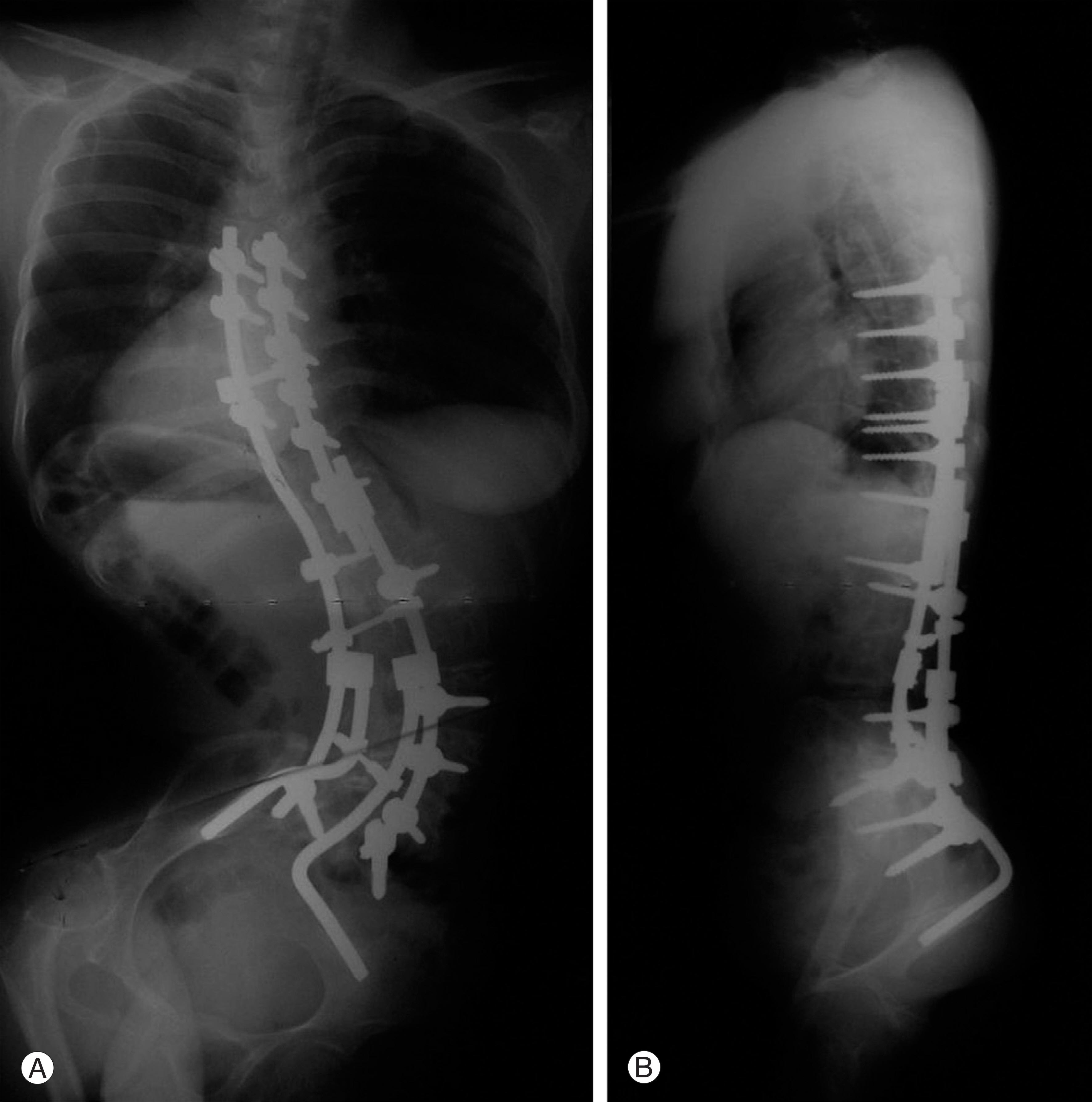
Fig. 1. (A, B) Galveston L-rod technique. Galveston rods were used to fix pelvis for residual poliomyelitis patient with paralytic scoliosis. Rods were connected to upper spine rods of pedicle screw system with parallel rod connectors.

Fig. 2. (A, B) Iliac screw fixation for neuromuscular scoliosis. Iliac screws make strongest fixation to ilium and easier connection to rod with offset connectors. However, prominence of iliac screw head should be avoided carefully.

Fig. 3. (A, B) Sub-S1 alar screw. Alar screws were added to enhance fixation of sacrum for patient with tubrculous spondylitis of L5 body after corpectomy and femoral shaft allograft. S1 pedicle screws were not enough for sacral fixation due to osteoporosis.
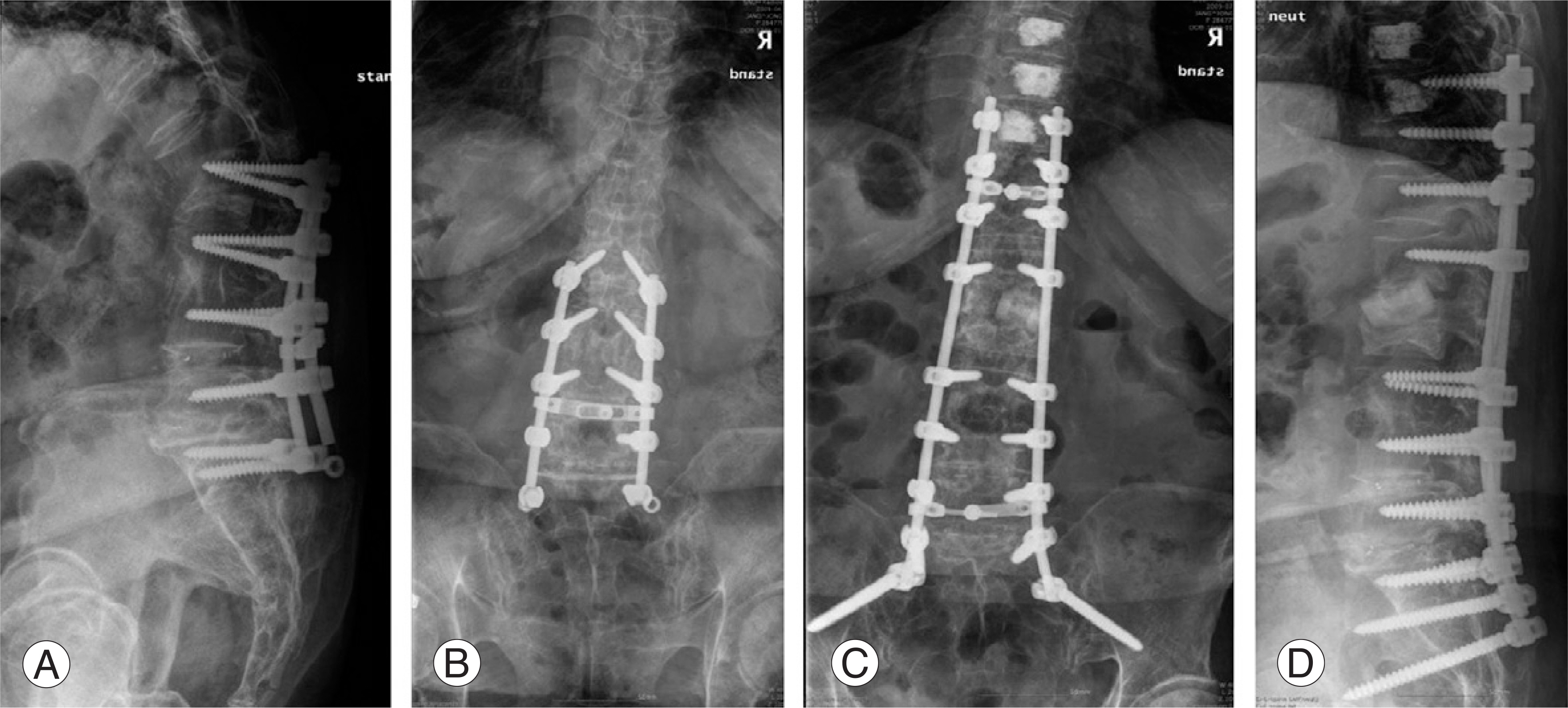
Fig. 4. Iliac screw fixation for revision surgery. (A, B) Following several operations, implant fixation failure at the lower end and junctional kyphosis at the upper end had developed. (C, D) Revision with iliac screws and extension of proximal fixation were performed.

Fig. 5. (A, B) L5-S1 transdiscal screw. For high grade spondylolisthesis, anterior transdiscal and four alar screws were applied.

Fig. 6. (A, B) Iliac crest rod. Tumor was resected from left sacroiliac joint. Iliac crest rod was applied with iliac screw to enhance iliac fixation.
Cited by 1 articles
-
Treatment of Unstable Sacral Fractures Related to Spino-Pelvic Dissociations
Hong-Sik Kim, Jung-Hwan Lee, Ki-Chul Park, Ye-Soo Park
J Korean Fract Soc. 2013;26(3):178-183. doi: 10.12671/jkfs.2013.26.3.178.
Reference
-
01). Smith SA., Abitol J., Carlson GD., Anderson DR., Tag-gart KW., Garfin SR. The effects of depth of penetration, screw orientation, and bone density on sacral screw fixation. Spine. 1993. 18:1006–1010.
Article02). Saer EH., Winter RB., Lonstein JE. Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine. 1990. 15:650–653.03). Boachie-Adjei O., Dendrinos GK., Ogilvie JW., Bradford DS. Management of adult spinal deformity with combined anterior-posterior arthrodesis and Luque-Galveston instrumentation. J Spinal Disord. 1991. 4:131–141.
Article04). Emami A., Deviren V., Berven S., Smith JA., Hu SS., Bradford DS. Outcome and complication of long fusion to the sacrum in adult spinal deformity: Luque-Galveston, combined iliac and sacral screws, and sacral fixation. Spine. 2002. 27:776–786.05). Kim YJ., Bridwell KH., Lenke LG., Rhim S., Cheh G. Pseudarthrosis in long adult spinal deformity instrumentation and fusion to the sacrum: Prevalence and risk factor analysis of 144 cases. Spine. 2006. 31:2329–2336.
Article06). Allen BI., Ferguson RL. The Galveston technique for L-rod instrumentation of the scoliotic spine. Spine. 1982. 7:276–284.07). McCord DH., Cunningham BW., Shono Y., Myers JJ., McAfee PC. Biomechanical analysis of lumbosacral fixation. Spine. 1992. 17:235–243.
Article08). Camp JF., Caudle R., Ashman RD., Rouch J. Immediate complication of Cotrel-Dubousset instrumentation to the sacro-pelvis: A clinical and biomechanical study. Spine. 1990. 15:932–941.09). Yazici M., Asher MA., Mardacker JW. The safety and efficacy of Isola-Galveston instrumentation and arthrodesis in the treatment of neuromuscular spinal deformities. J Bone Joint Surg Am. 2000. 82:524–543.
Article10). McCarthy RE., Dunn H., McCullough FL. Luque fixation to the sacral alar using the Dunn-McCarthy modification. Spine. 1989. 14:281–284.11). Walick KS., King JT., Johnston CE., Rathjen KE. Neuropathic lower extremity pain following Dunn-McCarthy Instrumentation. Spine. 2008. 33:877–880.
Article12). Peelle MW., Lenke LG., Bridwell KH., Sides B. Comparison of pelvic fixation techniques in neuromuscular spinal deformity correction: Galveston rod versus iliac and lumbosacral screws. Spine. 2006. 31:2392–2398.
Article13). Tsuchiya K., Bridwell KH., Kuklo TR., Lenke LG., Bal-dus C. Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine. 2006. 31:303–308.
Article14). Kostuik JP., Valdevit A., Chang HG., Kanzaki K. Biomechanical testing of the lumbosacral spine. Spine,. 1998. 23:1721–1728.
Article15). Jackson RP., McManus AC. The iliac buttress. A computed tomographic study of sacral anatomy. Spine. 1993. 18:1318–1328.16). Minamide A., Akamaru T., Yoon ST., Tamaki T., Rhee JM., Hutton WC. Transdiscal L5-S1 screws for the fixation of isthmic spondylolisthesis: A biomechanical evaluation. J Spinal Disord. 2003. 16:144–149.
Article17). Farcy W., Rawlins BA., Glassman SD. Technique and results of fixation to the sacrum with iliosacral screw. Spine. 1992. 17:190–195.18). Routt MLC., Nork SE., Mills WJ. Percutaneous fixation of pelvic ring disruptions. Clin Orthop Relat Res. 2000. 375:15–29.
Article19). Asher MA. Lumbopelvic fixation with the Isola spinal implant system. Margulies JY, Floman Y, Farcy JPC, Neuwirth MG, editors. Lumbosacral and spinopelvic fixation. New York: Lippincott-Raven;p. 215. 1996.20). Phillips JH., Gutheil JP., Knapp DR. Iliac screw fixation in neuromuscular scoliosis. Spine. 2007. 32:1566–1570.
Article21). Zhang HY., Thongtrangan I., Balabhadra RS., Murovic JA., Kim DH. Surgical technique for total sacrectomy and spinopelvic reconstruction. Neurosurg Focus. 2003. 15:5–14.22). O'Brien JR., Yu WD., Bhatnagar R., Sponseller P., Kebaish KM. An anatomic study of the S2 iliac technique for lumbopelvic screw placement. Spine. 2009. 34:349–442.23). Chang TL., Sponseller PD., Kebaish KM., Fishman EK. Low profile pelvic fixation: Anatomical parameters for sacral alar-iliac fixation versus traditional iliac fixation. Spine. 2009. 34:436–440.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changes of Spinopelvic Parameter using Iliac Screw In Surgical Correction of Sagittal Imbalance Patients
- Complications of Iliac Screw in Spinopelvic Fixation With Adult Spinal Deformity: Complications of Iliac Screw in Spinopelvic Fixation
- Lumbopelvic Fixation with Iliac Screw in Spinopelvic Dissociation
- Management of Sacral Tumors Requiring Spino-Pelvic Reconstruction with Different Histopathologic Diagnosis: Evaluation with Four Cases
- Impact of Spinal Correction Surgeries with Osteotomy and Pelvic Fixation in Patients with Kyphosis Due to Osteoporotic Vertebral Fractures
