Autosomal Dominant Polycystic Kidney Disease Combined with Intracranial Aneurysm and Dilated Cardiomyopathy: A Case Report
- Affiliations
-
- 1Department of Radiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea. smchong@cau.ac.kr
- 2Division of Cardiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
- 3Department of Neurosurgery, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea.
- KMID: 1819785
- DOI: http://doi.org/10.3348/jksr.2014.71.2.84
Abstract
- Extrarenal manifestations of autosomal dominant polycystic kidney disease (ADPKD) include non-renal, various intracranial, and cardiac cysts. A 26-year-old man with presumed ADPKD was also diagnosed with hemoptysis and dyspnea. The chest radiograph and CT scans indicated bilateral consolidations, ground-glass opacities, and bilateral pleural effusions, indicating symptoms of pulmonary edema. Based on the systolic dysfunction, left atrial enlargement, and left ventricular enlargement by echocardiography, he was diagnosed with dilated cardiomyopathy (DCMP). On screening brain CT angiography, an intracranial aneurysm (ICA) was detected in the right middle cerebral artery. Although the reason of a strong connection between ADPKD and DCMP is still unclear apart from the connection between ADPKD and ICA, DCMP may be considered as another cardiovascular manifestation of ADPKD when idiopathic DCMP is diagnosed in a patient with ADPKD.
MeSH Terms
-
Adult
Angiography
Brain
Cardiomyopathy, Dilated*
Deoxycytidine Monophosphate
Dyspnea
Echocardiography
Hemoptysis
Humans
Intracranial Aneurysm*
Mass Screening
Middle Cerebral Artery
Pleural Effusion
Polycystic Kidney, Autosomal Dominant*
Pulmonary Edema
Radiography, Thoracic
Tomography, X-Ray Computed
Deoxycytidine Monophosphate
Figure
-
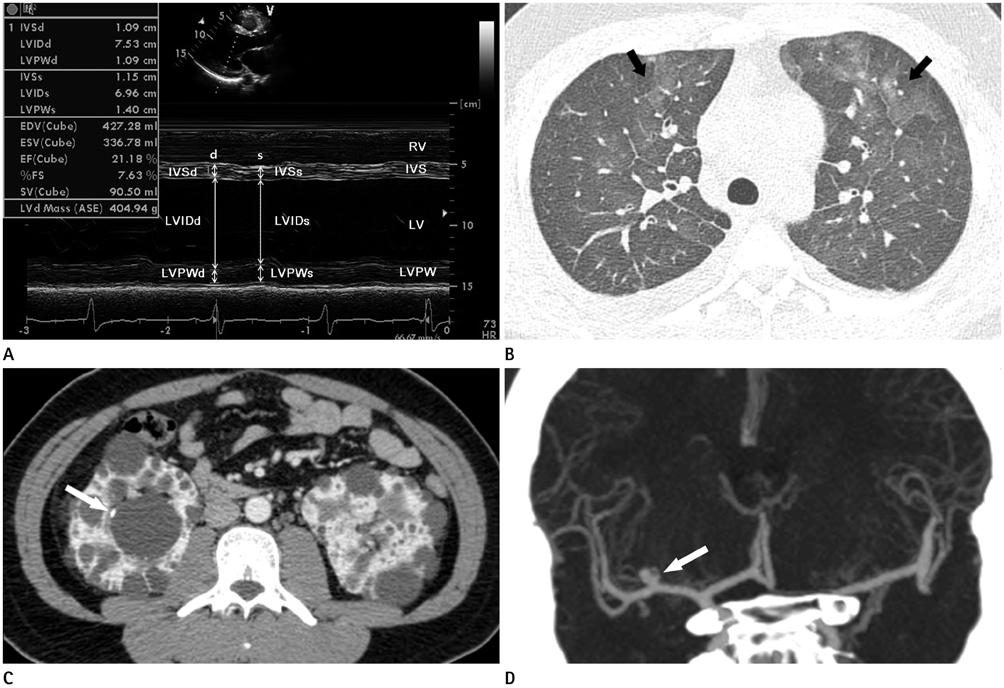
Fig. 1 Autosomal dominant polycystic kidney disease combined with intracranial aneurysm and dilated cardiomyopathy in a 26-year-old male patient. A. M-mode view from parasternal long axis view of echocardiography shows abnormally increased LVIDd and LVIDs, suggesting marked LV dilation and global hypokinesia of LV wall. Calculated EF reveals severe systolic dysfunction (EF = 21%). B. Lung window image of initial chest CT scan at level of aortic arch shows diffuse ground glass opacity with interlobular septal thickening in both lungs (arrows), suggesting pulmonary edema. C. Contrast enhanced abdominal CT scan demonstrates numerous small and large renal cysts in both kidneys. Note a large cyst with wall calcification in the right kidney (arrow). D. Maximal intensity projection image of initial brain CT angiography reveals a saccular aneurysm in the M1 segment of right MCA, measuring 4 mm (arrow). Note.-d = diastole, EDV = end diastolic volume, EF = ejection fraction, ESV = end systolic volume, IVS = interventricular septum, LV = left ventricle, LVd Mass = left ventricular mass at end diastole, LVID = left ventricular internal diameter, LVPW = left ventricular posterior wall, RV = right ventricle, s = systole, SV = stroke volume, %FS = percent fractional shortening
Reference
-
1. Martinez JR, Grantham JJ. Polycystic kidney disease: etiology, pathogenesis, and treatment. Dis Mon. 1995; 41:693–765.2. Luciano RL, Dahl NK. Extra-renal manifestations of autosomal dominant polycystic kidney disease (ADPKD): considerations for routine screening and management. Nephrol Dial Transplant. 2014; 29:247–254.3. Handa SP. Cardiovascular manifestations of autosomal dominant polycystic kidney disease in young adults. Clin Invest Med. 2006; 29:339–346.4. Torres VE. Extrarenal manifestations of autosomal dominant polycystic kidney disease. Am J Kidney Dis. 1999; 34:xlv–xlviii.5. Rahbari-Oskoui F, Mittal A, Mittal P, Chapman A. Renal relevant radiology: radiologic imaging in autosomal dominant polycystic kidney disease. Clin J Am Soc Nephrol. 2014; 9:406–415.6. Ecder T, Schrier RW. Cardiovascular abnormalities in autosomal-dominant polycystic kidney disease. Nat Rev Nephrol. 2009; 5:221–228.7. Griffin MD, Torres VE, Grande JP, Kumar R. Vascular expression of polycystin. J Am Soc Nephrol. 1997; 8:616–626.8. Nauser TD, Stites SW. Diagnosis and treatment of pulmonary hypertension. Am Fam Physician. 2001; 63:1789–1798.9. Parvari R, Levitas A. The mutations associated with dilated cardiomyopathy. Biochem Res Int. 2012; 2012:639250.10. Paavola J, Schliffke S, Rossetti S, Kuo IY, Yuan S, Sun Z, et al. Polycystin-2 mutations lead to impaired calcium cycling in the heart and predispose to dilated cardiomyopathy. J Mol Cell Cardiol. 2013; 58:199–208.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Dilated Cardiomyopathy Associated with Autosomal Dominant Polycystic Kidney Disease
- Polycystic Kidney Disease Presenting as Subarachnoid Hemorrhage Due to Ruptured Cerebral Aneurysm: An Autopsy Case
- A Case of Intramural Hematoma Coexisting with Autosomal Dominant Polycystic Kidney Disease and Intracranial Aneurysm
- Adult Polycystic Kidney Disease with Cardiovascular Assault
- A Case of Renal Cell Carcinoma in Autosomal Dominant Polycystic Kidney Disease Hemodialyzed
