CT Densitometry of the Lung in Healthy Nonsmokers with Normal Pulmonary Function
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. ejinchae@amc.seoul.kr
- 2Health Promotion Center, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 3Department of Pulmonary and Critical Care Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 1819749
- DOI: http://doi.org/10.3348/jksr.2012.67.5.341
Abstract
- PURPOSE
To investigate the upper normal limit of low attenuation area% in healthy nonsmokers.
MATERIALS AND METHODS
A total of 36 nonsmokers with normal pulmonary function test underwent a CT scan. Six thresholds (-980 - -930 HU) on inspiration CT and two thresholds (-950 and -910 HU) on expiration CT were used for obtaining low attenuation area%. The mean lung density was obtained on both inspiration CT and expiration CT. Descriptive statistics of low attenuation area% and the mean lung density, evaluation of difference of low attenuation area% and the mean lung density in both sex and age groups, analysis of the relationship between demographic information and CT parameters were performed.
RESULTS
Upper normal limit for low attenuation area% was 12.96% on inspiration CT (-950 HU) and 9.48% on expiration CT (-910 HU). Upper normal limit for the mean lung density was -837.58 HU on inspiration CT and 686.82 HU on expiration CT. Low attenuation area% and the mean lung density showed no significant differences in both sex and age groups. Body mass index (BMI) was negatively correlated with low attenuation area% on inspiration CT (-950 HU, r = -0.398, p = 0.016) and positively correlated with the mean lung density on inspiration CT (r = 0.539, p = 0.001) and expiration CT (r = 0.432, p = 0.009). Age and body surface area were not correlated with low attenuation area% or the mean lung density.
CONCLUSION
Low attenuation area% on CT densitometry of the lung could be found in healthy nonsmokers with normal pulmonary function, and showed negative association with BMI. Reference values, such as range and upper normal limit for low attenuation area% in healthy subjects could be helpful in quantitative analysis and follow up of early emphysema, using CT densitometry of the lung.
MeSH Terms
Figure
-
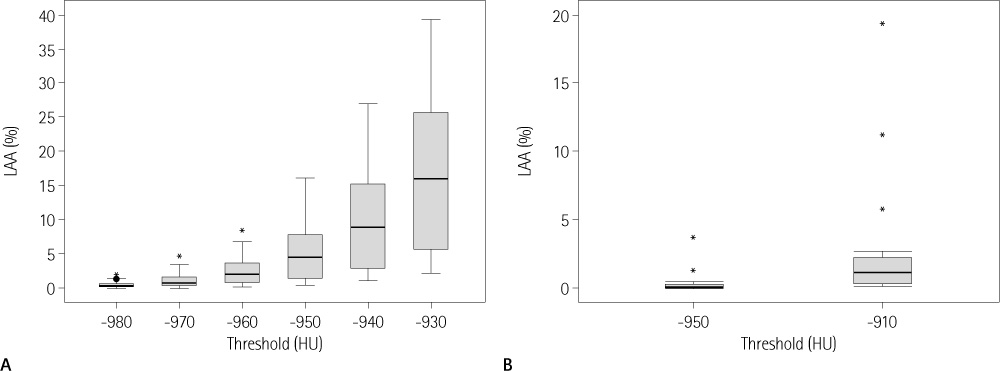
Fig. 1 Box and whisker plot of low attenuation area (%) along each thresholds on inspiratory CT (A) and expiratory CT (B). Note.-central line = median, ends of boxes = interquartile boundaries, whiskers = data point closest to inner fence (1.5 × interquartile range), • = mild outlier, * = severe outlier, HU = Hounsfield unit, LAA (%) = low attenuation area %

Fig. 2 Example of quantitative densitometry in a patient with mild emphysema and a healthy subject. A. A 54-year-old male who have mild degree of centrilobular emphysema. A coronal CT image (window level: -750 HU, width: 1500 HU) shows some areas of centrilobular emphysema in both upper lobes. Low attenuation area (%) is shown on a color-coded image demonstrating pixels having CT density below the threshold -950 HU and the value was 4.01%. B. A 59-year-old male who is one of healthy nonsmokers in this study. Emphysema is not evident on a coronal CT image (window level: -750 HU, width: 1500 HU). However, on a color-coded image, there are color-coded areas representing low attenuation area at -950 HU which value was 13.45%.
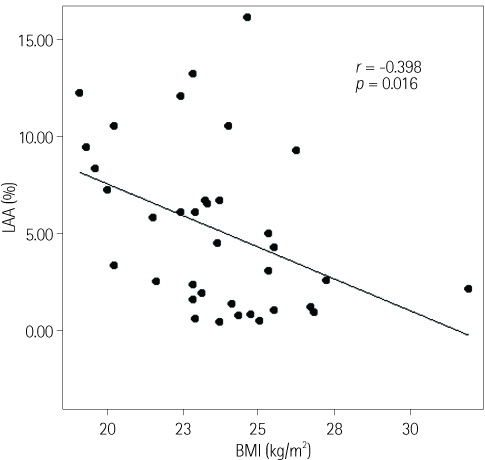
Fig. 3 Correlation between low attenuation area (%) at -950 HU on inspiration and body mass index. Note.-BMI = body mass index, LAA (%) = low attenuation area %
Reference
-
1. American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1995; 152(5 Pt 2):S77–S121.2. Bankier AA, De Maertelaer V, Keyzer C, Gevenois PA. Pulmonary emphysema: subjective visual grading versus objective quantification with macroscopic morphometry and thin-section CT densitometry. Radiology. 1999; 211:851–858.3. Gevenois PA, de Maertelaer V, De Vuyst P, Zanen J, Yernault JC. Comparison of computed density and macroscopic morphometry in pulmonary emphysema. Am J Respir Crit Care Med. 1995; 152:653–657.4. Gevenois PA, De Vuyst P, de Maertelaer V, Zanen J, Jacobovitz D, Cosio MG, et al. Comparison of computed density and microscopic morphometry in pulmonary emphysema. Am J Respir Crit Care Med. 1996; 154:187–192.5. Gevenois PA, De Vuyst P, Sy M, Scillia P, Chaminade L, de Maertelaer V, et al. Pulmonary emphysema: quantitative CT during expiration. Radiology. 1996; 199:825–829.6. Chae EJ, Seo JB, Song JW, Kim N, Park BW, Lee YK, et al. Slope of emphysema index: an objective descriptor of regional heterogeneity of emphysema and an independent determinant of pulmonary function. AJR Am J Roentgenol. 2010; 194:W248–W255.7. Kinsella M, Müller NL, Abboud RT, Morrison NJ, DyBuncio A. Quantitation of emphysema by computed tomography using a "density mask" program and correlation with pulmonary function tests. Chest. 1990; 97:315–321.8. Lee YK, Oh YM, Lee JH, Kim EK, Lee JH, Kim N, et al. Quantitative assessment of emphysema, air trapping, and airway thickening on computed tomography. Lung. 2008; 186:157–165.9. Müller NL, Staples CA, Miller RR, Abboud RT. "Density mask". An objective method to quantitate emphysema using computed tomography. Chest. 1988; 94:782–778.10. Park KJ, Bergin CJ, Clausen JL. Quantitation of emphysema with three-dimensional CT densitometry: comparison with two-dimensional analysis, visual emphysema scores, and pulmonary function test results. Radiology. 1999; 211:541–547.11. American Thoracic Society. Standardization of Spirometry, 1994 Update. Am J Respir Crit Care Med. 1995; 152:1107–1113.12. Stolk J, Putter H, Bakker EM, Shaker SB, Parr DG, Piitulainen E, et al. Progression parameters for emphysema: a clinical investigation. Respir Med. 2007; 101:1924–1930.13. Madani A, Zanen J, de Maertelaer V, Gevenois PA. Pulmonary emphysema: objective quantification at multi-detector row CT--comparison with macroscopic and microscopic morphometry. Radiology. 2006; 238:1036–1043.14. Lee HJ, Lee YK, Seo JB, Kim N, Oh YM, Lee SD. A study of the relationship between the pulmonary function test and the threshold value for the emphysema index at volumetric inspiration and expiration CT in cases of chronic obstructive lung disease. J Korean Radiol Soc. 2008; 59:99–106.15. Marsh S, Aldington S, Williams MV, Nowitz MR, Kingzett-Taylor A, Weatherall M, et al. Utility of lung density measurements in the diagnosis of emphysema. Respir Med. 2007; 101:1512–1520.16. Irion KL, Marchiori E, Hochhegger B, Porto Nda S, Moreira Jda S, Anselmi CE, et al. CT quantification of emphysema in young subjects with no recognizable chest disease. AJR Am J Roentgenol. 2009; 192:W90–W96.17. Stoel BC, Stolk J. Optimization and standardization of lung densitometry in the assessment of pulmonary emphysema. Invest Radiol. 2004; 39:681–688.18. Stolk J, Ng WH, Bakker ME, Reiber JH, Rabe KF, Putter H, et al. Correlation between annual change in health status and computer tomography derived lung density in subjects with alpha1-antitrypsin deficiency. Thorax. 2003; 58:1027–1030.19. Gevenois PA, Scillia P, de Maertelaer V, Michils A, De Vuyst P, Yernault JC. The effects of age, sex, lung size, and hyperinflation on CT lung densitometry. AJR Am J Roentgenol. 1996; 167:1169–1173.20. Gillooly M, Lamb D. Airspace size in lungs of lifelong non-smokers: effect of age and sex. Thorax. 1993; 48:39–43.21. Ogawa E, Nakano Y, Ohara T, Muro S, Hirai T, Sato S, et al. Body mass index in male patients with COPD: correlation with low attenuation areas on CT. Thorax. 2009; 64:20–25.22. Coxson HO, Chan IH, Mayo JR, Hlynsky J, Nakano Y, Birmingham CL. Early emphysema in patients with anorexia nervosa. Am J Respir Crit Care Med. 2004; 170:748–752.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical use of chest CT in chronic obstructive pulmonary diseases
- Quantification of Emphysema with a Three-Dimensional Chest CT Scan: Correlation with the Visual Emphysema Scoring on Chest CT, Pulmonary Function Tests and Dyspnea Severity
- Inspiratory and Expiratory HRCT Findings in Healthy Smokers' Lung
- Idiopathic Pulmonary Fibrosis with Coexisting Emphysema: High-Resolution CT and Clinical Correlation
- Measurement of Lung Volumes: Usefulness of Spiral CT
