Intra-arterial Onyx Embolization of Vertebral Body Lesions
- Affiliations
-
- 1Department of Radiology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USA.
- 2Department of Neurological Surgery, Brigham and Women's Hospital and Harvard Medical School, Boston, MA, USA. bgross1@partners.org
- 3Division of Neurological Surgery, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USA.
- KMID: 1810792
- DOI: http://doi.org/10.7461/jcen.2013.15.4.320
Abstract
- While Onyx embolization of cerebrospinal arteriovenous shunts is well-established, clinical researchers continue to broaden applications to other vascular lesions of the neuraxis. This report illustrates the application of Onyx (eV3, Plymouth, MN) embolization to vertebral body lesions, specifically, a vertebral hemangioma and renal cell carcinoma vertebral body metastatic lesion.
Keyword
MeSH Terms
Figure
-
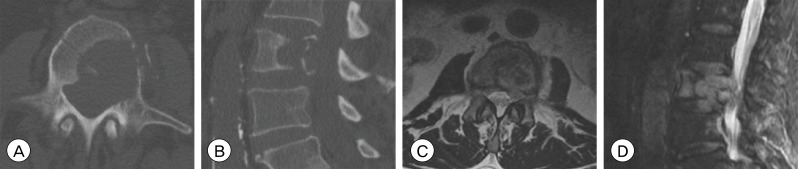
Fig. 1 Axial noncontrast lumbar spine computed tomography (A) and sagittal reformat (B) show a destructive L2 lesion with extension into the left pedicle and large epidural soft tissue component causing moderate spinal canal stenosis. There is pathologic compression with at least 50% loss of height centrally. Axial (C) and sagittal (D) T2 magnetic resonance images demonstrate a large destructive L2 lesion with pathologic fracture and 4 mm soft tissue extension into the ventral spinal canal, resulting in moderate left sided spinal canal narrowing.

Fig. 2 Selective angiography of the left L2 segmental artery demonstrates a significant pathologic vascular blush at the level of the L2 vertebral body (A). Post-embolization unsubtracted radiograph shows Onyx distributed diffusely through the lateral vertebral body (B). Post-embolization selective left L2 segmental artery injection demonstrates grossly total angiographic devascularization of the L2 vertebral body tumor (C).
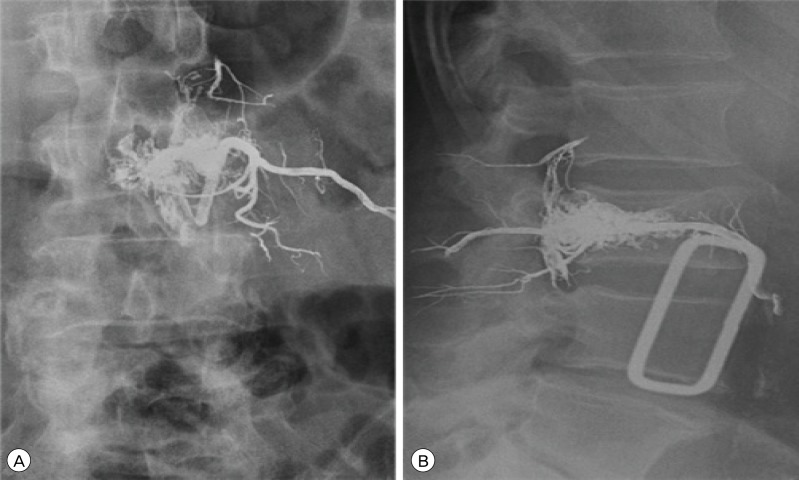
Fig. 3 Postembolization frontal (A) and lateral (B) lumbar spine radiographs show penetration of Onyx through tumor vessels within the L2 vertebral body. Reflux into the epidural venous plexus is seen.
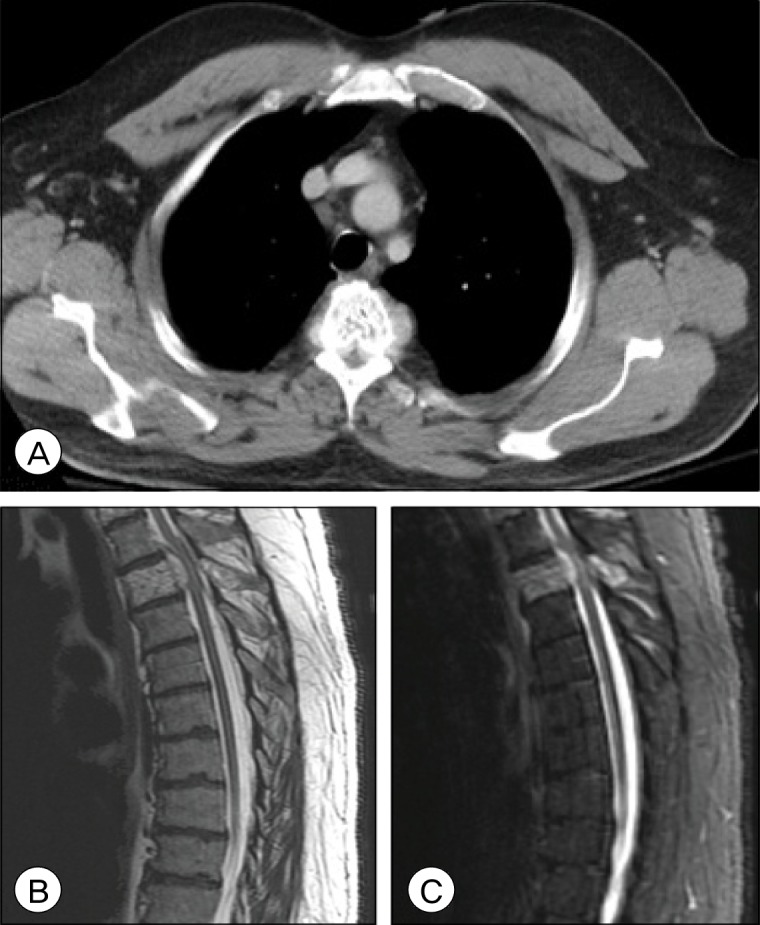
Fig. 4 Axial computed tomography demonstrates a hypodense lesion with coarse trabeculae within the T3 vertebral body with extensive soft tissue in the surrounding paravertebral and epidural space causing significant anterior cord compression (A). Sagittal T2-weighted (B) and Short T1 Inversion Recovery (STIR) (C) magnetic resonance images of thoracic spine demonstrate a heterogeneous lesion at the T3 vertebral body extending laterally and posteriorly through the vertebral body and causing severe central canal compression.
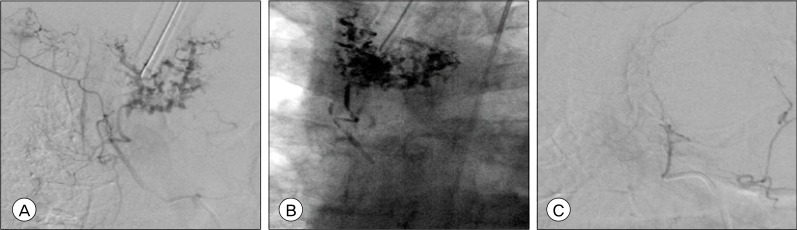
Fig. 5 Selective angiography of the right T4 segmental artery demonstrates a pathologic blush in the region of the T3 vertebral body (A). Intraprocedural unsubtracted antero-posterior radiograph demonstrates Onyx distributed through the known T3 hemangioma (B). Post-embolization selective injection of the right T4 segmental artery demonstrates no residual opacification of the pathologic vascular blush (C).
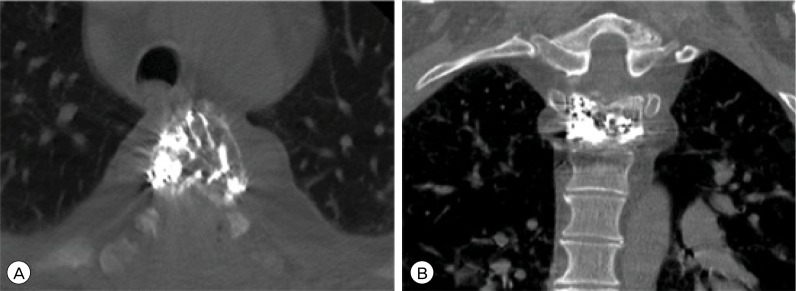
Fig. 6 Postembolization axial noncontrast computed tomography (A) and coronal reformat (B) show penetration of Onyx through tumor vessels within the T3 vertebral body.
Reference
-
1. Acosta FL Jr, Dowd CF, Chin C, Tihan T, Ames CP, Weinstein PR. Current treatment strategies and outcomes in the management of symptomatic vertebral hemangiomas. Neurosurgery. 2006; 2. 58(2):287–295. discussion 287-95. PMID: 16462482.
Article2. Berkefeld J, Scale D, Kirchner J, Heinrich T, Kollath J. Hypervascular spinal tumors: Influence of the embolization technique on perioperative hemorrhage. AJNR Am J Neuroradiol. 1999; 5. 20(5):757–763. PMID: 10369341.3. Clarençon F, Di Maria F, Cormier E, Sourour NA, Enkaoua E, Sailhan F, et al. Onyx injection by direct puncture for the treatment of hypervascular spinal metastases close to the anterior spinal artery: Initial experience. J Neurosurg Spine. 2013; 6. 18(6):606–610. PMID: 23600580.
Article4. Elhammady MS, Wolfe SQ, Ashour R, Farhat H, Moftakhar R, Lieber BB, et al. Safety and efficacy of vascular tumor embolization using Onyx: Is angiographic devascularization sufficient? J Neurosurg. 2010; 5. 112(5):1039–1045. PMID: 19698039.
Article5. Fox MW, Onofrio BM. The natural history and management of symptomatic and asymptomatic vertebral hemangiomas. J Neurosurg. 1993; 1. 78(1):36–45. PMID: 8416240.
Article6. Hurley MC, Gross BA, Surdell D, Shaibani A, Muro K, Mitchell CM, et al. Preoperative Onyx Embolization of Aggressive Vertebral Hemangiomas. AJNR Am J Neuroradiol. 2008; 6. 29(6):1095–1097. PMID: 18372419.
Article7. Kim LJ, Albuquerque FC, Aziz-Sultan A, Spetzler RF, McDougall CG. Low morbidity associated with the use of NBCA liquid adhesive for preoperative transarterial emoblization of central nervous system tumors. Neurosurgery. 2006; 7. 59(1):98–104. discussion 98-104. PMID: 16823305.8. Krueger EG, Sobel GL, Weinstein C. Vertebral hemangioma with compression of spinal cord. J Neurosurg. 1961; 5. 18:331–338. PMID: 13754556.
Article9. Lang EK, Sullivan J. Management of primary and metastatic renal cell carcinoma by transcatheter embolization with iodine 125. Cancer. 1988; 7. 62(2):274–282. PMID: 3383128.
Article10. Laredo JD, Reizine D, Bard M, Merland JJ. Vertebral hemangiomas: Radiologic evaluation. Radiology. 1986; 10. 161(1):183–189. PMID: 3763864.
Article11. Manke C, Bretschneider T, Lenhart M, Strotzer M, Neumann C, Gmeinwieser J, et al. Spinal metastases from renal cell carcinoma: Effect of preoperative particle embolization on intraoperative blood loss. AJNR Am J Neuroradiol. 2001; 5. 22(5):997–1003. PMID: 11337348.12. Smith TP, Koci T, Mehringer CM, Tsai FY, Fraser KW, Dowd CF, et al. Transarterial embolization of vertebral hemangioma. J Vasc Interv Radiol. 1993; Sep-Oct. 4(5):681–685. PMID: 8219564.
Article13. Sundaresan N, Galicich JH, Lane JM, Bains MS, McCormack P. Treatment of neoplastic epidural cord compression by vertebral body resection and stabilization. J Neurosurg. 1985; 11. 63(5):676–684. PMID: 4056870.
Article14. Sundaresan N, Scher H, DiGiacinto GV, Yagoda A, Whitmore W, Choi IS. Surgical treatment of spinal cord compression in kidney cancer. J Clin Oncol. 1986; 12. 4(12):1851–1856. PMID: 2431111.
Article15. Sundaresan N, Choi IS, Hughes JE, Sachdev VP, Berenstein A. Treatment of spinal metastases from kidney cancer by presurgical embolization and resection. J Neurosurg. 1990; 10. 73(4):548–554. PMID: 2398386.
Article16. Swanson DA, Orovan WL, Johnson DE, Giacco G. Osseous metastases secondary to renal cell carcinoma. Urology. 1981; 12. 18(6):556–561. PMID: 7314355.
Article17. Thakur NA, Daniels AH, Schiller J, Valdes MA, Czerwein JK, Schiller A, et al. Benign tumors of the spine. J Am Acad Orthop Surg. 2012; 11. 20(11):715–724. PMID: 23118137.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hairball-Like Migration of “Onyx Threads” into the Draining Vein during Transarterial Embolization of a Dural Arteriovenous Fistula: A Case Report and Experimental Validation
- Complication Associated with Onyx Embolization of Spinal Cord Arteriovenous Malformation
- Foreign body granuloma reaction after endovascular therapy of an unruptured right frontal arteriovenous malformation
- Preoperative Embolization of Cerebellar Hemangioblastoma with Onyx: Report of Three Cases
- Transvenous Onyx embolization of cavernous sinus dural arteriovenous fistula using a balloon catheter in the arterial side for flow control
