MRI Findings on Iatrogenic Spinal Infection Following Various Pain Management Procedures
- Affiliations
-
- 1Department of Radiology, Dankook University Hospital, Cheonan, Korea. jyleee@dankook.ac.kr
- 2Department of Orthopedic Surgery, Dankook University Hospital, Cheonan, Korea.
- KMID: 1801552
- DOI: http://doi.org/10.3348/jksr.2014.71.6.296
Abstract
- PURPOSE
The aim of this study was to investigate and report magnetic resonance imaging (MRI) findings of iatrogenic spinal infection (ISI).
MATERIALS AND METHODS
We retrospectively reviewed the clinical and MRI findings on 18 patients diagnosed with ISI. The MRI findings were evaluated for the number of spinal segments showing inflammation in the longitudinal span and affected vertebral bodies and discs, the presence of abscess in the epidural or paravertebral space, paravertebral myositis, and skip lesions.
RESULTS
Among the 18 patients, the range of the longitudinal span of spinal inflammation was 2-11 (mean = 5.84) vertebral segments. 17 of the 18 patients had three or more contiguous vertebral segments. The osteomyelitis and disc destruction was apparent in 77.8% and 66.7% of the patients, and 78% of patients with osteomyelitis showed involvement of one or two vertebrae; 91.7% of patients with disc destruction showed involvement of single disc. The incidence of epidural or paravertebral abscesses, and paravertebral myositis were 88.9%, and 94.4%. There were no spinal skip lesions.
CONCLUSION
MRI findings of those are wide longitudinal span of infection, involvement of no more than one or two vertebral bodies and a single disc, large abscesses, extensive myositis and no skip lesions, can be a useful ISI-diagnostic tool.
MeSH Terms
Figure
-

Fig. 1 Iatrogenic spinal infection following laser discectomy for L5-S1 with aggravated back pain in 55-year-old man. A. Sagittal fat-suppressed enhanced T1-weighted image shows diffuse enhancement in L5 and S1 vertebral bodies with anterior and posterior subligamentous extensions. Large multiloculated abscesses in the epidural space (arrowheads) extend longitudinally from the L3 to S2. B. Axial fat-suppressed enhanced T1-weighted image at the level of L5-S1 shows large multiloculated abscesses in the epidural space (arrowheads) and paravertebral space (arrows) with thin, smooth walls. In the muscles, inflammatory changes, including psoas, iliacus, multifidus, longissimus, and gluteus, are evident.

Fig. 2 Iatrogenic spinal infection following epidural anesthesia with febrile illness and back pain in 69-year-old woman. A. Sagittal MR images (T2-weighted, T1-weighted, fat-suppressed contrast-enhanced) show involvement of two vertebral bodies and one disc with disc destruction. Inflammatory changes are shown along the route of injection in the interspinous region of L3-4 (arrow). The longitudinal 10-vertebral-segment span of infection extends vertically from T11 to S3 (not shown here). B. Axial fat-suppressed enhanced T1-weighted image shows extensive myositis in the dorsal (thin arrows) and ventral (thick arrows) paravertebral spaces with multiple abscesses.
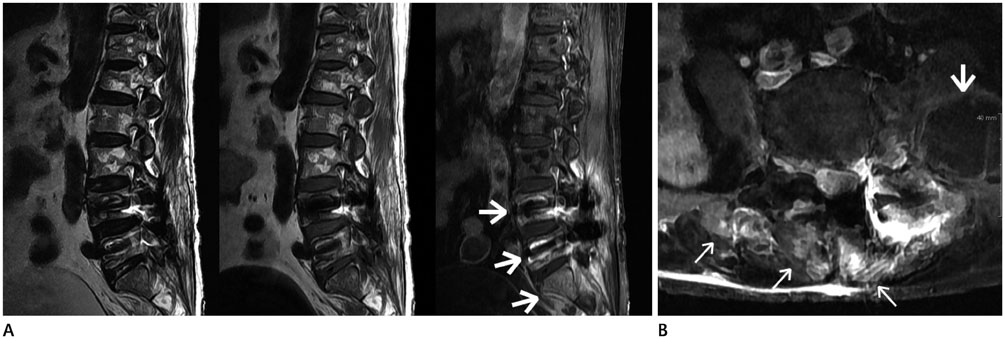
Fig. 3 Iatrogenic spinal infection following acupuncture with aggravated pain and fever in 74-year-old woman. A. Sagittal MR images (T2-weighted, T1-weighted, fat-suppressed contrast-enhanced) show involvement of three vertebral bodies (L4, L5, and S1, arrows) without involvement of intervening intervertebral discs. The longitudinal 11-vertebral-segment extends vertically from T10 to S3 (not shown here). Image distortion by metal artifacts in the L4 and L5 vertebrae from previous, eight-years-earlier spinal surgery is shown. B. Axial fat-suppressed enhanced T1-weighted image at the level of L4-5 shows large paravertebral abscess (thick arrow) and pyomyositis in the dorsal paravertebral space (thin arrows).

Fig. 4 Iatrogenic spinal infection following acupuncture with aggravated pain in 48-year-old woman. Sagittal MR images (T2-weighted, T1-weighted, fat-suppressed contrast-enhanced) show non-involvement of vertebral body or intervening intervertebral disc despite large epidural (arrowheads) and paravertebral (arrow) abscesses and wide longitudinal span of infection. The L5 body shows a chronic compression fracture and normal marrow signal intensity.
Reference
-
1. Epstein NE. The risks of epidural and transforaminal steroid injections in the Spine: commentary and a comprehensive review of the literature. Surg Neurol Int. 2013; 4:Suppl 2. S74–S93.2. McGrath JM, Schaefer MP, Malkamaki DM. Incidence and characteristics of complications from epidural steroid injections. Pain Med. 2011; 12:726–731.3. Zeidman SM, Thompson K, Ducker TB. Complications of cervical discography: analysis of 4400 diagnostic disc injections. Neurosurgery. 1995; 37:414–417.4. Trautmann M, Lepper PM, Schmitz FJ. Three cases of bacterial meningitis after spinal and epidural anesthesia. Eur J Clin Microbiol Infect Dis. 2002; 21:43–45.5. Sillevis Smitt P, Tsafka A, van den Bent M, de Bruin H, Hendriks W, Vecht C, et al. Spinal epidural abscess complicating chronic epidural analgesia in 11 cancer patients: clinical findings and magnetic resonance imaging. J Neurol. 1999; 246:815–820.6. Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev. 2000; 23:175–204. discussion 205.7. Schütze M, Piek J. Paracervical abscesses as life-threatening complications of outpatient pain treatment. Report of three cases. Neurosurg Focus. 2004; 17:E13.8. Gaul C, Neundörfer B, Winterholler M. Iatrogenic (para-) spinal abscesses and meningitis following injection therapy for low back pain. Pain. 2005; 116:407–410.9. Modic MT, Feiglin DH, Piraino DW, Boumphrey F, Weinstein MA, Duchesneau PM, et al. Vertebral osteomyelitis: assessment using MR. Radiology. 1985; 157:157–166.10. Hong SH, Choi JY, Lee JW, Kim NR, Choi JA, Kang HS. MR imaging assessment of the spine: infection or an imitation? Radiographics. 2009; 29:599–612.11. Lee SW, Lee SH, Chung HW, Kim MJ, Seo MJ, Shin MJ. Candida spondylitis: comparison of MRI findings with bacterial and tuberculous causes. AJR Am J Roentgenol. 2013; 201:872–877.12. Greenspan A. Orthopedic imaging: a practical approach. 5th ed. Philadelphia: Lippincott Williams & Wilkins;2011. p. 789–819.13. Resnick D, Niwayama G. Osteomyelitis, septic arthritis, and soft tissue infection: the axial skeleton. In : Resnick D, editor. Diagnosis of bone and joint disorders. Philadelphia, PA: WB Saunders;2002. p. 2481–2509.14. Xu S, Wang L, Cooper E, Zhang M, Manheimer E, Berman B, et al. Adverse events of acupuncture: a systematic review of case reports. Evid Based Complement Alternat Med. 2013; 2013:581203.15. Kindler CH, Seeberger MD, Staender SE. Epidural abscess complicating epidural anesthesia and analgesia. An analysis of the literature. Acta Anaesthesiol Scand. 1998; 42:614–620.16. Pobiel RS, Schellhas KP, Pollei SR, Johnson BA, Golden MJ, Eklund JA. Diskography: infectious complications from a series of 12,634 cases. AJNR Am J Neuroradiol. 2006; 27:1930–1932.17. Alcock E, Regaard A, Browne J. Facet joint injection: a rare form cause of epidural abscess formation. Pain. 2003; 103:209–210.18. Lee JH, Cho JH, Jo DJ. Cervical epidural abscess after cupping and acupuncture. Complement Ther Med. 2012; 20:228–231.19. Kim SY, Han SH, Jung MW, Hong JH. Generalized infection following facet joint injection -A case report-. Korean J Anesthesiol. 2010; 58:401–404.20. Weingarten TN, Hooten WM, Huntoon MA. Septic facet joint arthritis after a corticosteroid facet injection. Pain Med. 2006; 7:52–56.21. Park MS, Moon SH, Hahn SB, Lee HM. Paraspinal abscess communicated with epidural abscess after extra-articular facet joint injection. Yonsei Med J. 2007; 48:711–714.22. Orpen NM, Birch NC. Delayed presentation of septic arthritis of a lumbar facet joint after diagnostic facet joint injection. J Spinal Disord Tech. 2003; 16:285–287.23. Byun YS, Kim HT, Chang SA, Lee SR, Hwang DH, Kim SH. Iatrogenic spinal infection after injection therapy in spine. J Korean Soc Spine Surg. 2006; 13:299–305.24. Lindner A, Warmuth-Metz M, Becker G, Toyka VV. Iatrogenic spinal epidural abscesses: early diagnosis essential for good outcome. Eur J Med Res. 1997; 2:201–205.25. Kim SY, Hong SJ, Lee CY, Chung KB, Park CM. Tuberculous spondylitis vs pyogenic spondylitis: focusing on the discriminative MR findings for differentiation. J Korean Radiol Soc. 2007; 56:183–189.26. Jung NY, Jee WH, Ha KY, Park CK, Byun JY. Discrimination of tuberculous spondylitis from pyogenic spondylitis on MRI. AJR Am J Roentgenol. 2004; 182:1405–1410.27. Kapeller P, Fazekas F, Krametter D, Koch M, Roob G, Schmidt R, et al. Pyogenic infectious spondylitis: clinical, laboratory and MRI features. Eur Neurol. 1997; 38:94–98.28. Cheung WY, Luk KD. Pyogenic spondylitis. Int Orthop. 2012; 36:397–404.
