Imaging Sci Dent.
2014 Jun;44(2):165-169. 10.5624/isd.2014.44.2.165.
Clival lesion incidentally discovered on cone-beam computed tomography: A case report and review of the literature
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology, University of Connecticut School of Dental Medicine, Farmington, CT, USA. dr.aniket.jadhav@gmail.com
- 2Division of Diagnostic Sciences and Therapeutics, University of Connecticut School of Medicine, Farmington, CT, USA.
- KMID: 1799600
- DOI: http://doi.org/10.5624/isd.2014.44.2.165
Abstract
- An osteolytic lesion with a small central area of mineralization and sclerotic borders was discovered incidentally in the clivus on the cone-beam computed tomography (CBCT) of a 27-year-old male patient. This benign appearance indicated a primary differential diagnosis of non-aggressive lesions such as fibro-osseous lesions and arrested pneumatization. Further, on magnetic resonance imaging (MRI), the lesion showed a homogenously low T1 signal intensity with mild internal enhancement after post-gadolinium and a heterogeneous T2 signal intensity. These signal characteristics might be attributed to the fibrous tissues, chondroid matrix, calcific material, or cystic component of the lesion; thus, chondroblastoma and chondromyxoid fibroma were added to the differential diagnosis. Although this report was limited by the lack of final diagnosis and the patient lost to follow-up, the incidental skull base finding would be important for interpreting the entire volume of CBCT by a qualified oral and maxillofacial radiologist.
Keyword
MeSH Terms
Figure
-

Fig. 1 A. A panoramic radiograph of the patient shows increased ramal height on right side. B. A posterio-anterior skull view shows facial asymmetry and deviated jaw.

Fig. 2 SPECT study shows very mild uptake in the right mandibular condyle.

Fig. 3 A. Axial CBCT shows osteolytic lesion on clivus with hyperostotic borders and small area of mineralization internally. B. Coronal image shows lateral extent of the lesion and sclerotic rim. C. Sagittal image shows anterio-posterior extension of the lesion.
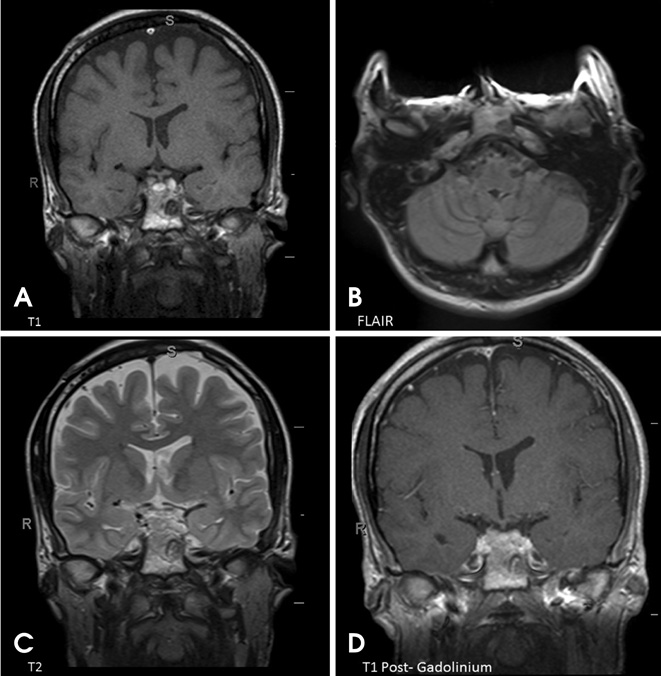
Fig. 4 A and B. Coronal T1 weighted (A) and axial FLAIR MR images show low signal intensity. C. Coronal T2 weighted image shows heterogeneous intensity internally. D. Coronal T1 post gadolinium image shows very mild internal enhancement.
Reference
-
1. Alhadidi A, Cevidanes LH, Paniagua B, Cook R, Festy F, Tyndall D. 3D quantification of mandibular asymmetry using the SPHARM-PDM tool box. Int J Comput Assist Radiol Surg. 2012; 7:265–271.
Article2. Swennen GR, Mollemans W, Schutyser F. Three-dimensional treatment planning of orthognathic surgery in the era of virtual imaging. J Oral Maxillofac Surg. 2009; 67:2080–2092.
Article3. Price JB, Thaw KL, Tyndall DA, Ludlow JB, Padilla RJ. Incidental findings from cone beam computed tomography of the maxillofacial region: a descriptive retrospective study. Clin Oral Implants Res. 2012; 23:1261–1268.
Article4. Laine FJ, Nadel L, Braun IF. CT and MR imaging of the central skull base. Part 1: Techniques, embryologic development, and anatomy. Radiographics. 1990; 10:591–602.
Article5. Chaljub G, Van Fleet R, Guinto FC Jr, Crow WN, Martinez L, Kumar R. MR imaging of clival and paraclival lesions. AJR Am J Roentgenol. 1992; 159:1069–1074.
Article6. Welker KM, DeLone DR, Lane JI, Gilbertson JR. Arrested pneumatization of the skull base: imaging characteristic. AJR Am J Roentgenol. 2008; 190:1691–1696.7. Bloch OG, Jian BJ, Yang I, Han SJ, Aranda D, Ahn BJ, et al. Cranial chondrosarcoma and recurrence. Skull Base. 2010; 20:149–156.
Article8. Borges A. Skull base tumours: Part II. Central skull base tumours and intrinsic tumours of the bony skull base. Eur J Radiol. 2008; 66:348–362.9. Douis H, Saifuddin A. The imaging of cartilaginous bone tumours. II. Chondrosarcoma. Skeletal Radiol. 2013; 42:611–626.
Article10. Géhanne C, Delpierre I, Damry N, Devroede B, Brihaye P, Christophe C. Skull base chordoma: CT and MRI features. JBR-BTR. 2005; 88:325–327.11. Wein RO, Popat SR, Doerr TD, Dutcher PO. Plasma cell tumors of the skull base: four case reports and literature review. Skull Base. 2002; 12:77–86.
Article12. Borges A. Imaging of the central skull base. Neuroimaging Clin N Am. 2009; 19:669–696.
Article13. Ben Salem D, Allaoui M, Dumousset E, Ponnelle T, Justrabo E, Martin D, et al. Chondroblastoma of the temporal bone associated with a persistent hypoglossal artery. Acta Neurochir (Wien). 2002; 144:1315–1318.14. Hatano M, De Donato G, Falcioni M, Sanna M. Chondroblastoma of the temporal bone. Acta Otolaryngol. 2011; 131:890–895.
Article15. Dran G, Niesar E, Vandenbos F, Noel G, Paquis P, Lonjon M. Chondroblastoma of the apex portion of petrousal bone. Childs Nerv Syst. 2007; 23:231–235.
Article16. Weber AL. Imaging of the skull base. Eur J Radiol. 1996; 22:68–81.
Article17. Scarfe WC, Li Z, Aboelmaaty W, Scott SA, Farman AG. Maxillofacial cone beam computed tomography: essence, elements and steps to interpretation. Aust Dent J. 2012; 57:Suppl 1. 46–60.
Article18. Berland LL, Silverman SG, Gore RM, Mayo-Smith WW, Megibow AJ, Yee J, et al. Managing incidental findings on abdominal CT: white paper of the ACR incidental findings committee. J Am Coll Radiol. 2010; 7:754–773.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Foramen transversarium enlargement caused by vertebral artery tortuosity: Diagnosis with cone-beam computed tomography and magnetic resonance angiography
- Detection of maxillary second molar with two palatal roots using cone beam computed tomography: a case report
- Cone beam computed tomography findings of ectopic mandibular third molar in the mandibular condyle: report of a case
- Isolated tympanic plate fracture detected by cone-beam computed tomography: report of four cases with review of literature
- Cone beam CT findings of retromolar canals: Report of cases and literature review
