Stanford Type A Aortic Dissection Secondary to Infectious Aortitis: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 2Department of Thoracic and Cardiovascular Surgery, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. minhoki@naver.com
- 3Department of Radiology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 1786951
- DOI: http://doi.org/10.3346/jkms.2013.28.3.485
Abstract
- Nowadays, infectious aortitis has become a rare disease thanks to antibiotics, but remains life-threatening. We present a case of a patient with acupuncture-induced infectious aortitis leading to aortic dissection. Chest computed-tomogram scan revealed Stanford type A dissection with pericardial effusion. Under the impression of an impending rupture, emergent surgery was performed. During surgery, infectious aortitis was identified incidentally, so she underwent resection of the infected aorta including surrounding tissues. Then the ascending aorta and hemi-arch were replaced with a prosthetic graft as an in situ fashion. The resected tissue and blood cultures revealed Staphylococcus aureus, so prolonged antibiotherapy was prescribed.
Keyword
MeSH Terms
Figure
-
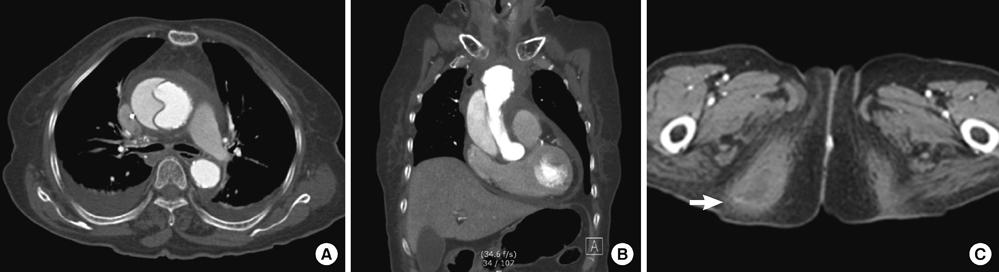
Fig. 1 Enhanced chest CT scans with axial (A) and coronal images (B) show the dissection flap of the ascending aorta with pericardial effusion and wall thickening of the proximal aortic arch, which may be suggested a soft tissue infection or hematoma. Mediastinal fluid collection and bilateral pleural effusion are also noted. (C) Abscess on the right buttock (white arrow) was found incidentally at CT scans.
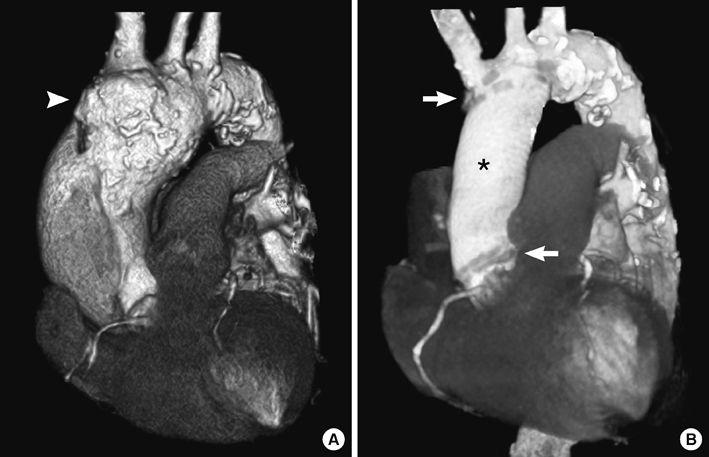
Fig. 2 Pre-operative (A) and post-operative (B) three-dimensional volume rendering of contrast-enhanced CT scans. (A) Preoperative CT scans show Stanford type A aortic dissection with the enlarged ascending aorta and that the proximal aortic arch was aneurysmal and atherosclerous changes. During surgery, infectious aortitis was identified incidentally at the proximal aortic arch (arrowhead). (B) Postoperative chest CT scans revealed that the ascending aorta and hemiarch were replaced with a prosthetic graft (asterisk) and patent. Also proximal and distal anastomotic lines (arrow) were visible.
Reference
-
1. Lao L, Hamilton GR, Fu J, Berman BM. Is acupuncture safe? a systematic review of case reports. Altern Ther Health Med. 2003. 9:72–83.2. Lee S, Lim SH, Kim DK, Joo HC. Acupuncture induced necrotizing aortitis with infected pseudoaneurysm formation. Yonsei Med J. 2008. 49:322–324.3. Long R, Guzman R, Greenberg H, Safneck J, Hershfield E. Tuberculous mycotic aneurysm of the aorta: review of published medical and surgical experience. Chest. 1999. 115:522–531.4. Oderich GS, Panneton JM, Bower TC, Cherry KJ Jr, Rowland CM, Noel AA, Hallett JW Jr, Gloviczki P. Infected aortic aneurysms: aggressive presentation, complicated early outcome, but durable results. J Vasc Surg. 2001. 34:900–908.5. Lopes RJ, Almeida J, Dias PJ, Pinho P, Maciel MJ. Infectious thoracic aortitis: a literature review. Clin Cardiol. 2009. 32:488–490.6. Gornik HL, Creager MA. Aortitis. Circulation. 2008. 117:3039–3051.7. Ting AC, Cheng SW, Ho P, Poon JT, Tsu JH. Surgical treatment of infected aneurysms and pseudoaneurysms of the thoracic and abdominal aorta. Am J Surg. 2005. 189:150–154.8. Foote EA, Postier RG, Greenfield RA, Bronze MS. Infectious aortitis. Curr Treat Options Cardiovasc Med. 2005. 7:89–97.9. Malouf JF, Chandrasekaran K, Orszulak TA. Mycotic aneurysms of the thoracic aorta: a diagnostic challenge. Am J Med. 2003. 115:489–496.10. Bronze MS, Shirwany A, Corbett C, Schaberg DR. Infectious aortitis: an uncommon manifestation of infection with Streptococcus pneumoniae. Am J Med. 1999. 107:627–630.11. Maillet JM, Palombi T, Sablayrolles JL, Bonnet N. Septic rupture of an atherosclerotic plaque of the ascending aorta. Interact Cardiovasc Thorac Surg. 2012. 15:790–791.12. Bedeleanu D, Coman C, Encica S, Hagiu R, Molnar A, Cãpâlneanu R. Stanford type A aortic dissection in a hypertensive patient with atherosclerosis of aorta and aortitis. Echocardiography. 2000. 17:181–185.13. Choi JB, Yang HW, Oh SK, Yun KJ. Rupture of ascending aorta secondary to tuberculous aortitis. Ann Thorac Surg. 2003. 75:1965–1967.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retrograde Stanford type A aortic dissection after endovascular stent graft placement for type B dissection
- A Case of Idiopathic Aortitis Mimicking Severe Aortic Stenosis
- A Case of Aortic Dissection with Compromised Superior Mesenteric Artery Treated with Stents Insertion at Origin of the Artery
- A Case of Infectious Aortitis Causing Recurrent Acinetobacter baumannii Bacteremia Following Aortic Valve Replacement
- Retrograde Aortic Dissection after Thoracic Endovascular Aortic Repair for Descending Aorta: 2 case reports
