Newly Developed Multiple Myeloma in a Patient with Primary T-Cell Lymphoma of Bone
- Affiliations
-
- 1Department of Internal Medicine, Division of Hemato-Oncology, Chonnam National University Medical School, Gwangju, Korea. ijchung@chonnam.ac.kr
- KMID: 1786900
- DOI: http://doi.org/10.3346/jkms.2008.23.3.544
Abstract
- Primary non-Hodgkin's lymphoma of bone (PLB) is rare, and generally presents as a single extensive and destructive bone lesion. Histopathologically, most cases present as diffuse large B-cell lymphoma, and T-cell lymphoma is rare. By contrast, multiple myeloma is a disease defined as the neoplastic proliferation of a single clone of plasma cells producing a monoclonal immunoglobulin. We report a case of multiple myeloma that developed during treatment of PLB in a type of T-cell. A 48-yr-old man was diagnosed as T-cell PLB, stage IE, 18 months ago. The patient received the chemoradiotherapy and salvage chemotherapy for PLB. However, the lymphoma progressed with generalized bone pain, and laboratory findings showed bicytopenia and acute renal failure. On bone marrow biopsy, the patient was diagnosed as having multiple myeloma newly developed with primary T-cell lymphoma of bone. In spite of chemotherapy, the patient died of renal failure.
MeSH Terms
Figure
-

Fig. 1 Simple radiography showed osteolytic lesions in the right distal tibia (A). Magnetic resonance imaging (MRI) of the right ankle revealed a heterogeneous, extraosseous mass in the right tibia (B). The Tc-99m bone scan revealed diffuse hot uptake in the right tibia without any other bony involvement at the time of diagnosis of lymphoma (C).
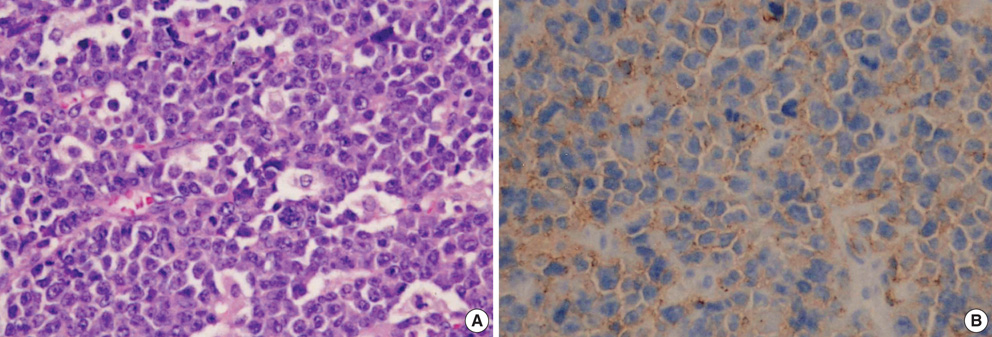
Fig. 2 Diffuse infiltration of large tumor cells with vesicular prominent nucleoli, abundant cytoplasm, and numerous mitotic cells (A, H&E, ×200). Immunohistochemical staining for CD45RO showed positive (B, ×200).
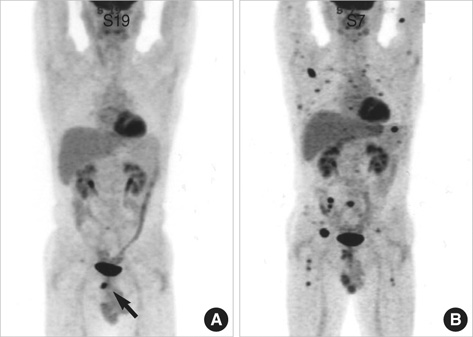
Fig. 3 After chemoradiotherapy, F-18 FDG PET-CT showed the residual hypermetabolic lesion on tibia, but also revealed hot uptakes at the inferior ramus of the right pubis (A). Despite salvage chemotherapy, F-18 FDG PET-CT revealed diffuse hot uptake in a skeletal area (B).
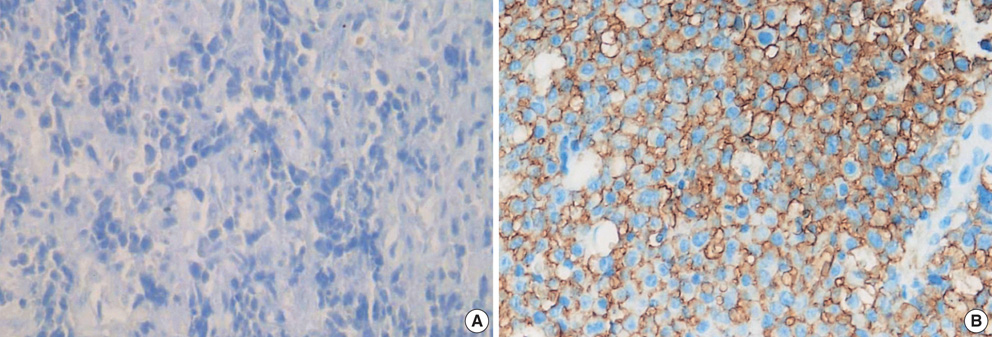
Fig. 4 CD138 expression in the lymphoma mass (A) and bone marrow biopsy at the diagnosis of multiple myeloma (B) (×200).
Reference
-
1. Dubey P, Ha CS, Besa PC, Fuller L, Cabanillas F, Murray J, Hess MA, Cox JD. Localized primary malignant lymphoma of bone. Int J Radiat Oncol Biol Phys. 1997. 37:1087–1093.
Article2. Gianelli U, Patriarca C, Moro A, Ponzoni M, Giardini R, Massimino M, Alfano RM, Armiraglio E, Nuciforo P, Bosari S, Coggi G, Parafioriti A. Lymphomas of the bone: a pathological and clinical study of 54 cases. Int J Surg pathol. 2002. 10:257–266.
Article3. Limb D, Dreghorn C, Murphy JK, Mannion R. Primary lymphoma of bone. Int Orthop. 1994. 18:180–183.
Article4. Ostrowski ML, Unni KK, Banks PM, Shives TC, Evans RG, O'Connell MJ, Taylor WF. Malignant lymphoma of bone. Cancer. 1986. 58:2646–2655.
Article5. Winkler RE, Ruchlemer R, Heyd J. Multifocal T-cell lymphoma of bone. Am J Hematol. 1999. 61:154.
Article6. Zinzani PL, Carrillo G, Ascani S, Barbieri E, Tani M, Paulli M, Stefoni V, Sabattini E, Alinari L, Binazzi R, Tura S, Baccarani M, Pileri SA. Primary bone lymphoma: experience with 52 patients. Haematologica. 2003. 88:280–285.7. Baar J, Burkes RL, Gospodarowicz M. Primary non-Hodgkin's lymphoma of bone. Semin Oncol. 1999. 26:270–275.8. Durr HR, Muller PE, Hiller E, Maier M, Baur A, Jansson V, Refior HJ. Malignant lymphoma of bone. Arch Orthop Trauma Surg. 2002. 122:10–16.
Article9. Heyning FH, Hogendoorn PC, Kramer MH, Hermans J, Kluin-Nelemans JC, Noordijk EM, Kluin PM. Primary non-Hodgkin's lymphoma of bone: a clinicopathological investigation of 60 cases. Leukemia. 1999. 13:2094–2098.
Article10. Mulligan ME, McRae GA, Murphey MD. Imaging features of primary lymphoma of bone. AJR Am J Roentgenol. 1999. 173:1691–1697.
Article11. Mendenhall NP, Jones JJ, Kramer BS, Hudson TM, Carter RL, Enneking WF, Marcus RB Jr, Million RR. The management of primary lymphoma of bone. Radiother Oncol. 1987. 9:137–145.
Article12. Fairbanks RK, Bonner JA, Inwards CY, Strickler JG, Habermann TM, Unni KK, Su J. Treatment of stage IE primary lymphoma of bone. Int J Radiat Oncol Biol Phys. 1994. 28:363–372.
Article13. Fidias P, Spiro I, Sobczak ML, Nielsen GP, Ruffolo EF, Mankin H, Suit HD, Harmon DC. Long term results of combined modality therapy in primary bone lymphomas. Int J Radiat Oncol Biol phys. 1999. 45:1213–1218.14. Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A, Fonseca R, Rajkumar SV, Offord JR, Larson DR, Plevak ME, Therneau TM, Greipp PR. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003. 78:21–33.
Article15. Lahtinen R, Laakso M, Palva I, Virkkunen P, Elomaa I. Randomised, placebo controlled multicentre trial of clodronate in multiple myeloma. Finnish Leukaemia Group. Lancet. 1992. 340:1049–1052.16. Blade J, Kyle RA. Multiple myeloma in young patients: Clinical presentation and treatment approach. Leuk Lymphoma. 1998. 30:493–501.17. A predictive model for aggressive non-Hodgkin's lymphoma. The International Non-Hodgkin's Lymphoma Prognostic Factors Project. N Engl J Med. 1993. 329:987–994.18. Bryant E, Ronan SG, Iossifides IA. Plasma cell myeloma in a patient with a cutaneous T-cell lymphoma. Cancer. 1982. 50:2122–2125.
Article19. Broder S, Poplack D, Whang-Peng J, Durm M, Goldman C, Muul L, Waldmann TA. Characterization of a suppressor cell leukemia: evidence for the requirement of an interaction of two T cells in the development of human suppressor effector cells. N Engl J Med. 1978. 298:66–72.20. Uchiyama T, Sagawa K, Takatsuki K, Uchino H. Effect of adult T cell leukemia cells on pokeweed mitogen-induced normal B-cell differentiation. Clin Immunol Immunopathol. 1978. 10:24–34.21. Wickenhauser C, Borchmann P, Diehl V, Scharffetter-Kochanek K. Development of IgG lambda multiple myeloma in a patient with cutaneous CD30+ anaplastic T-cell lymphoma. Leuk Lymphoma. 1999. 35:201–206.
