A Case of More Abundant and Dysplastic Adenomas in the Interposed Colon than in the Native Colon
- Affiliations
-
- 1Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea. leeyc@yuhs.ac
- 2Department of Pathology, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1786230
- DOI: http://doi.org/10.3349/ymj.2007.48.6.1075
Abstract
- We report a 60-year-old woman with intramucosal adenocarcinoma arising in the interposed colon, 40 years after the esophageal reconstruction for lye induced esophageal stricture. Although synchronous adenomas were also found in the native colon where the graft was taken, the number of adenomas was greater in the interposed colon and more dysplastic, even progressed to adenocarcinoma, than that of the native colon. The microsatellite instability-testing performed in the intramucosal carcinoma from interposed colon showed absence of microsatellite instability. Changing of location and functional deman]d of colonic segment, and the exposure to different intraluminal contents might have facilitated the adenoma- carcinoma transformation in the interposed colon.
MeSH Terms
Figure
-
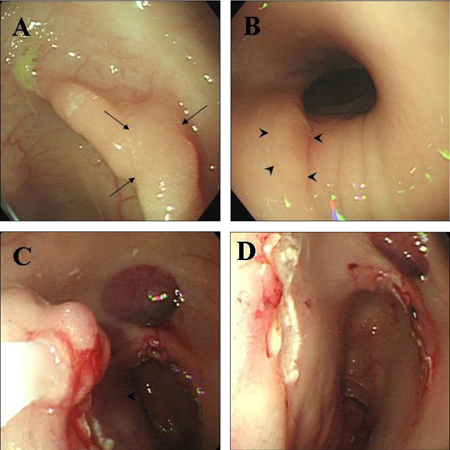
Fig. 1 (A, B, C, D) Arrows indicate the flat elevated mucosal lesion in the interposed colon, located at the anastomosis site and measuring 12 mm (A). Another flat elevated lesion located 4 cm proximal to the anastomosis site, measuring 20 mm is indicated with arrow heads (B). These polyps were removed by snare polypectomy after the submucosal injection of saline (C, D).

Fig. 2 (A, B) Pathology of the resected 20 mm sized adenoma showing tubulo-villous adenoma with high grade dysplasia and focus of intramucosal well-differentiated adenocarcinoma. (A × 100 and B × 400).
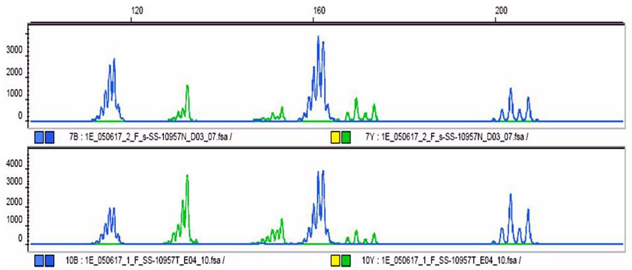
Fig. 3 The result of the MSI-testing using five microsatellite markers, BAT25, BAT 26, D2S123, D5S346 and D17S250, showed no shift of bands relative to control bands (upper: control, lower: specimen of patient).
Cited by 1 articles
-
Colonic Intramucosal Cancer in the Interposed Colon Treated with Endoscopic Mucosal Resection: A Case Report and Review of Literature
Seung-Ho Baek, Jang-Ho Lee, Dong Ryeol Yoo, Hye Yeong Kim, Meihua Jin, Ah-reum Jang, Dong-Hoon Yang, Jeong-Sik Byeon
Clin Endosc. 2019;52(4):377-381. doi: 10.5946/ce.2018.129.
Reference
-
1. Agha FP, Orringer MB. Colonic interposition: radiographic evaluation. AJR Am J Roentgenol. 1984. 142:703–708.2. Larson TC 3rd, Shuman LS, Libshitz HI, McMurtrey MJ. Complications of colonic interposition. Cancer. 1985. 56:681–690.3. Lundell L, Olbe L. Colonic interposition for reconstruction after resection of cancer in the esophagus and gastroesophageal junction. Eur J Surg. 1991. 157:189–192.4. Briel JW, Tamhankar AP, Hagen JA, DeMeester SR, Johansson J, Choustoulakis E, et al. Prevalence and risk factors for ischemia, leak, and stricture of esophageal anastomosis:gastric pull-up versus colon interposition. J Am Coll Surg. 2004. 198:536–542.5. Neagoe A, Molnar AM, Acalovschi M, Seicean A, Serban A. Risk factors for colorectal cancer: an epidemiologic descriptive study of a series of 333 patients. Rom J Gastroenterol. 2004. 13:187–193.6. Altorjay A, Kiss J, Vörös A, Szanto I, Bohak A. Malignant tumor developed in colon-esophagus. Hepatogastroenterology. 1995. 42:797–799.7. Bucknell A, Clark C. An experimental method for recording the behaviour of human isolated colonic segments. Gut. 1967. 8:569–573.8. Lindahl H, Rintala R, Sariola H, Louhimo I. Long-term endoscopic and flow cytometric follow-up of colon interposition. J Pediatr Surg. 1992. 27:859–861.9. Goldsmith HS, Beattie EJ Jr. Malignant villous tumor in a colon bypass. Ann Surg. 1968. 167:98–100.10. Licata AA, Fecanin P, Glowitz R. Metastatic adenocarcinoma from oesophageal colonic interposition. Lancet. 1978. 1:285.11. Haerr RW, Higgins EM, Seymore CH, el-Mahdi AM. Adenocarcinoma arising in a colonic interposition following resection of squamous cell esophageal cancer. Cancer. 1987. 60:2304–2307.12. Houghton AD, Jourdan M, McColl I. Dukes A carcinoma after colonic interposition for oesophageal stricture. Gut. 1989. 30:880–881.13. Theile DE, Smithers M, Strong RW, Windsor CJ. Primary adenocarcinoma in a colonic "oesophageal" segment. Aust N Z J Surg. 1992. 62:158–160.14. Lee SJ, Koay CB, Thompson H, Nicolaides AR, Das Gupta AR. Adenocarcinoma arising in an oesophageal colonic interposition graft. J Laryngol Otol. 1994. 108:80–83.15. Fritscher-Ravens A, Sriram PV, Thonke F, Jaeckle S, Maydeo A, Soehendra N. Synchronous adenocarcinoma in the transposed colonic conduit after esophagectomy for squamous cell cancer: endoscopic palliative resection while awaiting surgery. Gastrointest Endosc. 1999. 50:852–854.16. Goyal M, Bang DH, Cohen LE. Adenocarcinoma arising in interposed colon: report of a case. Dis Colon Rectum. 2000. 43:555–558.17. Liau CT, Hsueh S, Yeow KM. Primary adenocarcinoma arising in esophageal colon interposition: report of a case. Hepatogastroenterology. 2004. 51:748–749.18. Jass JR. HNPCC and sporadic MSI-H colorectal cancer: a review of the morphological similarities and differences. Fam Cancer. 2004. 3:93–100.19. de la Chapelle A. Microsatellite instability. N Engl J Med. 2003. 349:209–210.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two intertwined compartments coexisting in sporadic conventional colon adenomas
- Colonic Intramucosal Cancer in the Interposed Colon Treated with Endoscopic Mucosal Resection: A Case Report and Review of Literature
- Non-Surgical Management of Critically Compromised Airway Due to Dilatation of Interposed Colon
- Regression of colon polyposis after aspirin medication
- Hyperplastic Polyposis Associated with Two Synchronous Colon Cancers
