Corticosteroid Treatment in Siblings Affected with Severe Mycoplasma pneumoniae Pneumonia
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, The Catholic University of Korea, Seoul, Korea. leekyungyil@catholic.ac.kr
- 2Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 1782323
- DOI: http://doi.org/10.3947/ic.2009.41.3.190
Abstract
- Numerous evidences support the pathogenesis that M. pneumoniae pneumonia is associated with cell-mediated immune reaction. We report 2 cases of severe M. pneumoniae pneumonia in previously healthy sisters, who were both admitted during an epidemic of M.pneumoniae pneumonia. The elder sister, who was 16 years old, was admitted with M. pneumoniae pneumonia. She showed no response to treatment with clarithromycin and levofloxacin, and eventually progressed to severe ARDS, requiring mechanical ventilation. After treatment with hydrocortisone (200 mg/day), there were rapid improvements in clinical manifestations and chest radiographic findings. The younger sister, who was 14 years old, was admitted 10 days later, presenting with fever but no pneumonic lesions on chest radiograph. Just like her sister, the infection showed no response to clarithromycin. Fever persisted and pneumonic consolidation with mild pleural effusion was noticed in the left lower lobe on the 5th hospital-day. After treatment with oral prednisolone (1 mg/kg), she showed rapid defervescence and on the 8th hospital day, no pneumonic lesions were detectable on chest radiograph. Given the fact that the pathogenesis of pneumonia and extrapulmonary manifestations in M. pneumoniae infection is immune-mediated, an immunosuppressive therapy would be validated for selected patients with M. pneumoniae infections.
Keyword
MeSH Terms
Figure
-

Figure 1 Chest X-ray findings of case-1. A) Initial chest radiograph shows multifocal pneumonic consolidations in both lung fields with left pleural effusion. B) Further progression of extensive pneumonic consolidations and pleural effusion in both lung fields are present on the 3rd hospital day. C) Chest X-ray shows markedly improved lung lesions after corticosteroid therapy on the 8th hospital day.
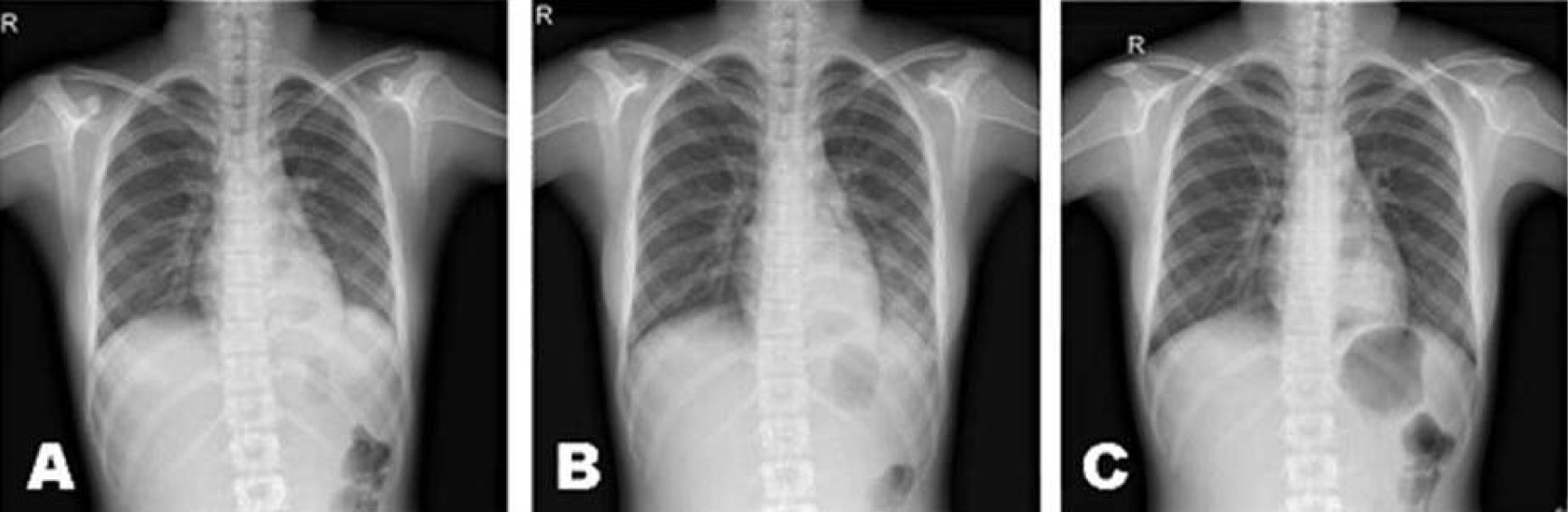
Figure 2 Chest X-ray findings of case-2. A) Initial chest radiograph shows no definitive pneumonic consolidation in both lung fields except suspicious increased density on left retrocadiac region. B) Fine reticular pneumonic consolidation in left lower lobe with mild blunting of costopleural angle is shown on the 4th hospital day. C) There is resolution of pneumonic consolidation after corticosteroid therapy on the 7th hospital day.
Cited by 2 articles
-
Early Additional Immune-Modulators for Mycoplasma pneumoniae Pneumonia in Children: An Observation Study
You-Sook Youn, Sung-Churl Lee, Jung-Woo Rhim, Myung-Seok Shin, Jin-Han Kang, Kyung-Yil Lee
Infect Chemother. 2014;46(4):239-247. doi: 10.3947/ic.2014.46.4.239.Mycoplasma pneumoniae Pneumonia Unresponsive to Macrolide Treatment
Misuk Ji, Heungsup Sung, Tae Sun Shim, Woori Jang, Mi-Na Kim
Lab Med Online. 2012;2(4):226-231. doi: 10.3343/lmo.2012.2.4.226.
Reference
-
1. Waites KB, Talkington DE. Mycoplasma pneumoniae and its role as a human pathogen. Clin Microbiol Rev. 2004. 17:697–728.
Article2. Dorigo-Zetsma JW, Wilbrink B, van der Nat H, Bartelds AI, Heijnen ML, Dankert J. Results of molecular detection of Mycoplasma pneumoniae among patients with acute respiratory infection and in their household contacts reveals children as human reservoirs. J Infect Dis. 2001. 183:675–678.
Article3. Chan ED, Welsh CH. Fulminant Mycoplasma pneumoniae pneumonia. West J Med. 1995. 162:133–142.4. Radisic M, Torn A, Gutierrez P, Defranchi HA, Pardo P. Severe acute lung injury caused by Mycoplasma pneumoniae: potential role for steroid pulses in treatment. Clin Infect Dis. 2000. 31:1507–1511.
Article5. Miyashita N, Obase Y, Ouchi K, Kawasaki K, Kawai Y, Kobayashi Y, Oka M. Clinical features of severe Mycoplasma pneumoniae pneumonia in adults admitted to an intensive care unit. J Med Microbiol. 2007. 56:1625–1629.
Article6. Lee KY, Lee HS, Hong JH, Lee MH, Lee JS, Burgner D, Lee BC. Role of prednisolone treatment in severe Mycoplasma pneumoniae pneumonia in children. Pediatr Pulmonol. 2006. 41:263–268.
Article7. Tamura A, Matsubara K, Tanaka T, Nigami H, Yura K, Fukaya T. Methylprednisolone pulse therapy for refractory Mycoplasma pneumoniae pneumonia in children. J Infect. 2008. 57:223–228.
Article8. Lee KY. Pediatric respiratory infections by Mycoplasma pneumoniae. Expert Rev AntiInfect Ther. 2008. 6:509–521.9. Kang KS, Woo HO. Pattern of occurrence of Mycoplasma pneumoniae pneumonia in admitted children: sourthen central Korea, from 1989 to 2002. J Korean Pediatr Soc. 2003. 46:474–479.10. Lee SH, Noh SM, Lee KY, Lee HS, Hong JH, Lee MH, Lee JS, Lee BC, Lee JS. Clinico-epidemiologic study of Mycoplasma pneumoniae pneumonia (1993 through 2003). Korean J Pediatr. 2005. 48:154–157.11. Layani-Milon MP, Gras I, Valette M, Luciani J, Stagnara J, Aymard M, Lina B. Incidence of upper respiratory tract Mycoplasma pneumoniae infections among outpatients in Rhône-Alpes, France, during five successive winter periods. J Clin Microbiol. 1999. 37:1721–1726.
Article12. Klement E, Talkington DF, Wasserzug O, Kayouf R, Davidovitch N, Dumke R, Bar-Zeev Y, Ron M, Boxman J, Lanier Thacker W, Wolf D, Lazarovich T, Shemer-Avni Y, Glikman D, Jacobs E, Grotto I, Block C, Nir-Paz R. Identification of risk factors for infection in an outbreak of Mycoplasma pneumoniae respitatory track disease. Clin Infect Dis. 2006. 43:1239–1245.
Article13. Cunha BA. The clinical diagnosis of Mycoplasma pneumoniae: the diagnostic importance of highly elevated serum cold agglutinins. Eur J Clin Microbiol Infect Dis. 2008. 27:1017–1019.
Article14. Loens K, Ursi D, Goossens H, Ieven M. Molecular diagnosis of Mycoplasma pneumoniae respiratory tract infections. J Clin Microbiol. 2003. 41:4915–4923.
Article15. McCracken GH Jr. Current status of antibiotic treatment for Mycoplasma pneumoniae infections. Pediatr Infect Dis. 1986. 5:167–171.
Article16. Sabato AR, Cooper DM, Thong YH. Transitory depression of immune function following Mycoplasma pneumoniae infection in children. Pediatr Res. 1981. 15:813–816.17. Starr S, Berkovich S. Effects of measles, gamma-globulin-modified measles and vaccine measles on the tuberculin test. N Engl J Med. 1964. 270:386–391.
Article18. Tagliabue C, Salvatore CM, Techasaensiri C, Mejias A, Torres JP, Katz K, Gomez AM, Esposito S, Principi N, Hardy RD. The impact of steroids given with macrolide therapy on experimental Mycoplasma pneumoniae infection. J Infect Dis. 2008. 198:1180–1188.
Article19. Tai DY. Pharmacologic treatment of SARS: current knowledge and recommendations. Ann Acad Med Singapore. 2007. 36:438–443.20. McGowan JE Jr, Chesney PJ, Crossley KB, LaForce FM. Guidelines for the use of systemic glucocorticosteroids in the management of selected infections. Working group on steroid use, antimicrobial agents committee, Infectious Diseases Society of America. J Infect Dis. 1992. 165:1–13.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mycoplasma pneumoniae Pneumonia in Children
- Clinical Observation on Pneumonia due to Mycoplasma Pneumoniae in Children
- A clinical study of mycoplasma pneumonia in children during recent 5 years
- Clinical Consideration on Pneumonia caused by Mycoplasma Pneumoniae in Children
- Clinical Study of Patients with Mycoplasma Pneumoniae Pneumonia in Children
