The First Korean Case of Camurati-Engelmann Disease (Progressive Diaphyseal Dysplasia) Confirmed by TGFB1 Gene Mutation Analysis
- Affiliations
-
- 1Department of Laboratory Medicine, Yonsei University College of Medicine, Seoul, Korea. KAL1119@yuhs.ac
- 2Department of Radiology, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1779212
- DOI: http://doi.org/10.3346/jkms.2009.24.4.737
Abstract
- Camurati-Engelmann disease (CED) is an autosomal dominant progressive diaphyseal dysplasia caused by mutations in the transforming growth factor-beta1 (TGFB1) gene. We report the first Korean family with an affected mother and son who were diagnosed with CED. The proband is a 19-yr-old male with a history of abnormal gait since the age of 2. He also suffered from proximal muscle weakness, pain in the extremities, and easy fatigability. Skeletal radiographs of the long bones revealed cortical, periosteal, and endosteal thickenings, predominantly affecting the diaphyses of the upper and lower extremities. No other bony abnormalities were noted in the skull and spine and no remarkable findings were seen on laboratory tests. The patient's mother had a long-standing history of mild limb pain. Under the impression of CED on radiographic studies, we performed mutation analysis. A heterozygous G to A transition at cDNA position +653 in exon 4 of the TGFB1 gene (R218H) was detected in the patient and his mother.
Keyword
MeSH Terms
Figure
-
Fig. 1 Family pedigree of this study. The arrow indicates the proband.
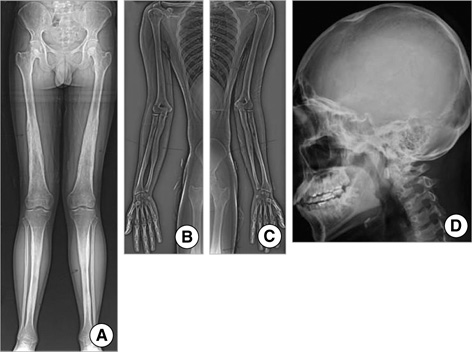
Fig. 2 Standing AP radiograph of the lower limbs (A), scannograms of the right (B) and left (C) upper limb, and right lateral view of the skull (D) of the proband. Cortical and periosteal thickenings confined to the diaphyses are seen in all long bones. Gross bony abnormalities were not seen in the skull.

Fig. 3 AP scannogram of the lower extremity of the proband's mother. Cortical and periosteal thickening with sclerosis confined to the diaphyses is also noted. Mild undermodeling is seen in the distal femurs and proximal tibias.
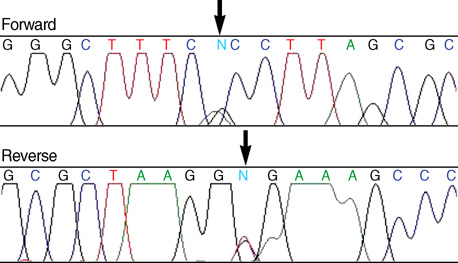
Fig. 4 Direct sequencing of exon 4 of the TGFB1 gene of the proband shows a heterozygous transition at cDNA position +653 (R218H). This mutation in the TGFB1 gene was detected in both the proband and his mother.
Reference
-
1. Janssens K, Vanhoenacker F, Bonduelle M, Verbruggen L, Van Maldergem L, Ralston S, Guanabens N, Migone N, Wientroub S, Divizia MT, Bergmann C, Bennett C, Simsek S, Melancon S, Cundy T, Van Hul W. Camurati-Engelmann disease: review of the clinical, radiological, and molecular data of 24 families and implications for diagnosis and treatment. J Med Genet. 2006. 43:1–11.
Article2. Wallace SE, Lachman RS, Mekikian PB, Bui KK, Wilcox WR. Marked phenotypic variability in progressive diaphyseal dysplasia (Camurati-Engelmann disease): report of a four-generation pedigree, identification of a mutation in TGFB1, and review. Am J Med Genet. 2004. 129A:235–247.
Article3. Simsek S, Janssens K, Kwee L, Van Hul W, Veenstra J, Netelenbos JC. Camurati-Englemann disease (progressive diaphyseal dysplasia) in a Moroccan family. Osteoporos Int. 2005. 16:1167–1170.4. Vanhoenacker FM, Janssens K, Van Hul W, Gershoni-Baruch R, Brik R, De Schepper AM. Camurati-Engelmann disease. Review of radioclinical features. Acta Radiol. 2003. 44:430–434.
Article5. Brat HG, Hamoir X, Matthijs P, Lambin P, Van Campenhoudt M. Camurati-Engelmann disease: a late and sporadic case with metaphyseal involvement. Eur Radiol. 1999. 9:159–162.
Article6. Janssens K, Gershoni-Baruch R, Van Hul E, Brik R, Guanabens N, Migone N, Verbruggen LA, Ralston SH, Bonduelle M, Van maldergem L, Vanhoenacker F, Van Hul W. Localisation of the gene causing diaphyseal dysplasia Camurati-Engelmann to chromosome 19q13. J Med Genet. 2000. 37:245–249.
Article7. Kinoshita A, Saito T, Tomita H, Makita Y, Yoshida K, Ghadami M, yamada K, Kondo S, Ikegawa S, Nishimura G, Fukushima Y, Nakagomi T, Saito H, Sugimoto T, Kamegaya M, hisa K, Murray JC, Taniguchi N, Niikawa N, Yoshiura K. Domain-specific mutations in TGFB1 result in Camurati-Engelmann disease. Nat Genet. 2000. 26:19–20.
Article8. Campos-Xavier B, Saraiva JM, Savarirayan R, Verloes A, Feingold J, Faivre L, Munnich A, Le Merrer M, Cormier-Daire V. Phenotypic variability at the TGF-beta1 locus in Camurati-Engelmann disease. Hum Genet. 2001. 109:653–658.9. Grey AC, Wallace R, Crone M. Engelmann's disease: a 45-year follow-up. J Bone Joint Surg Br. 1996. 78:488–491.10. Saraiva JM. Progressive diaphyseal dysplasia: a three-generation family with markedly variable expressivity. Am J Med Genet. 1997. 71:348–352.
Article11. Saraiva JM. Anticipation in progressive diaphyseal dysplasia. J Med Genet. 2000. 37:394–395.
Article12. Janssens K, ten Dijke P, Ralston SH, Bergmann C, Van Hul W. Transforming growth factor-beta 1 mutations in Camurati-Engelmann disease lead to increased signaling by altering either activation or secretion of the mutant protein. J Biol Chem. 2003. 278:7718–7724.13. Hecht JT, Blanton SH, Broussard S, Scott A, Rhoades Hall C, Milunsky JM. Evidence for locus heterogeneity in the Camurati-Engelmann (DPD1) syndrome. Clin Genet. 2001. 59:198–200.
Article
