Preoperative Radiologic and Postoperative Pathologic Risk Factors for Early Intra-Hepatic Recurrence in Hepatocellular Carcinoma Patients Who Underwent Curative Resection
- Affiliations
-
- 1Department of Diagnostic Radiology, Institute of Gastroenterology, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea. radpms@yuhs.ac
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Surgery, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1777092
- DOI: http://doi.org/10.3349/ymj.2009.50.6.789
Abstract
- PURPOSE
The risk of hepatocellular carcinoma (HCC) recurrence must be considered ahead of surgery. This study was undertaken to identify pre-operative risk factors for early intrahepatic recurrence of HCC after curative resection in a large-scale.
MATERIALS AND METHODS
We retrospectively reviewed the preoperative three-phase multi-detector CT (MDCT) and laboratory data for 240 HCC patients who underwent curative resection; tumor size, number, gross shape, capsule integrity, distinctiveness of tumor margin, portal vein thrombosis (PVT), alpha-fetoprotein level (AFP), and protein induced by vitamin K absence-II (PIVKA-II) levels were assessed. Surgical pathology was reviewed; tumor differentiation, capsule, necrosis, and micro-vessel invasion were recorded.
RESULTS
HCC recurred in 61 patients within six months (early recurrence group), but not in 179 patients (control group). In univariate analysis, large tumor size (p = 0.018), shape (p = 0.028), poor capsule integrity (p = 0.046), elevated AFP (p = 0.015), and PIVKA-II (p = 0.008) were significant preoperative risk factors. Among the pathologic features, PVT (p = 0.023), Glisson's capsule penetration (p = 0.033), microvascular invasion (p < 0.001), and poor differentiation (p = 0.001) showed statistical significance. In multivariate analysis, only the histopathologic parameters of microvascular invasion and poor differentiation achieved statistical significance.
CONCLUSION
Preoperative CT and laboratory parameters showed limited value, while the presence of microscopic vascular tumor invasion and poorly differentiated HCC correlated with higher risk of early recurrence after curative resection.
Keyword
MeSH Terms
-
Adult
Aged
Carcinoma, Hepatocellular/metabolism/pathology/*radiography/*surgery
Female
Humans
Liver Neoplasms/metabolism/pathology/*radiography/*surgery
Male
Middle Aged
Neoplasm Recurrence, Local/metabolism/*pathology/*radiography
Retrospective Studies
Risk Factors
Tomography, X-Ray Computed
alpha-Fetoproteins/metabolism
Figure
-
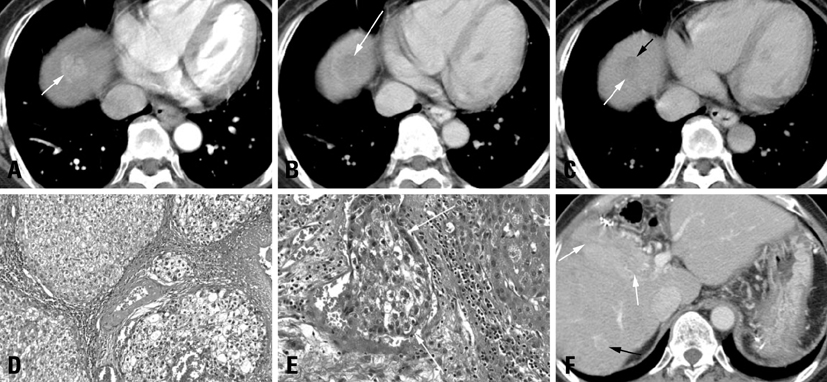
Fig. 1 A 56-year-old female with early recurrent HCC after segmentectomy. The AFP level in a blood sample obtained on the same day as the CT scan was 1076.84 IU/mL. (A) Arterial phase of the preoperative CT obtained by a 4-slice MDCT. A mass measuring approximately 2.2 cm in diameter which was later proven by surgery to be hepatocellular carcinoma is observed at the dome of the liver, presenting as a multinodular confulent nodule (arrow). (B) Early washout (arrow) of contrast of this nodule is observed during the portal venous phase, an enhancement pattern consistent with HCC. (C) The equilibrium phase of the preoperative CT. A linear enhancement structure (black arrow) was noted which was considered to be the radiological capsule. The radiological capsule was assessed to cover less than 25% of the tumor circumference (capsule grade 4). The margin of the nodule is poorly defined (white arrow). (D) Microscopic findings show high grade (Edmondson-Steiner grade III) hepatocellular carcinoma; original magnification, ×200; hematoxylin-eosin (H & E). (E) Microscopic examination revealed frequent microvessel tumor invasion (white arrows), original magnification, ×200; hematoxylin-eosin (H & E). (F) Marked increase of AFP level (10865.27 IU/mL) was observed at the fifth postoperative-month blood test. He underwent a CT scan, which revealed an infiltrative hypervascular mass (white arrow). Another 1 cm sized hypervascular nodule (black arrow) is noted, which increased further in size and measured to be 2.2 cm at a CT scan performed 4 months afterwards, and the findings were highly suggestive of a HCC nodule. HCC, hepatocellular carcinoma; MDCT, multi-detector CT.
Cited by 1 articles
-
Clinicopathological Characteristics in Combined Hepatocellular-Cholangiocarcinoma: A Single Center Study in Korea
Hana Park, Ki Hong Choi, Sae-Byeol Choi, Jong Won Choi, Do Young Kim, Sang Hoon Ahn, Kyung Sik Kim, Jin Sub Choi, Kwang-Hyub Han, Chae Yoon Chon, Jun Yong Park
Yonsei Med J. 2011;52(5):753-760. doi: 10.3349/ymj.2011.52.5.753.
Reference
-
1. Clark HP, Carson WF, Kavanagh PV, Ho CP, Shen P, Zagoria RJ. Staging and current treatment of hepatocellular carcinoma. Radiographics. 2005. 25:Suppl 1. S3–S23.
Article2. Ulmer SC. Hepatocellular carcinoma. A concise guide to its status and management. Postgrad Med. 2000. 107:117–124.3. Ng KK, Vauthey JN, Pawlik TM, Lauwers GY, Regimbeau JM, Belghiti J, et al. Is hepatic resection for large or multinodular hepatocellular carcinoma justified? Results from a multi-institutional database. Ann Surg Oncol. 2005. 12:364–373.
Article4. Mor E, Kaspa RT, Sheiner P, Schwartz M. Treatment of hepatocellular carcinoma associated with cirrhosis in the era of liver transplantation. Ann Intern Med. 1998. 129:643–653.
Article5. Bruix J, Llovet JM. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology. 2002. 35:519–524.
Article6. Fong Y, Sun RL, Jarnagin W, Blumgart LH. An analysis of 412 cases of hepatocellular carcinoma at a Western center. Ann Surg. 1999. 229:790–799.
Article7. Yamamoto J, Okada S, Shimada K, Okusaka T, Yamasaki S, Ueno H, et al. Treatment strategy for small hepatocellular carcinoma: comparison of long-term results after percutaneous ethanol injection therapy and surgical resection. Hepatology. 2001. 34:707–713.
Article8. Poon RT, Fan ST, Wong J. Selection criteria for hepatic resection in patients with large hepatocellular carcinoma larger than 10 cm in diameter. J Am Coll Surg. 2002. 194:592–602.
Article9. Hanazaki K, Kajikawa S, Shimozawa N, Shimada K, Hiraguri M, Koide N, et al. Hepatic resection for hepatocellular carcinoma in diameter of > or = 10 cm. Hepatogastroenterology. 2002. 49:518–523.10. Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, et al. Clinical management of hepatocellular carcinoma Conclusions of the Barcelona-2000 EASL conference European Association for the Study of the Liver. J Hepatol. 2001. 35:421–430.
Article11. Bolondi L, Gaiani S, Celli N, Golfieri R, Grigioni WF, Leoni S, et al. Characterization of small nodules in cirrhosis by assessment of vascularity: the problem of hypovascular hepatocellular carcinoma. Hepatology. 2005. 42:27–34.
Article12. Yamamoto M, Matsuda M, Iimuro Y, Fujii H, Nagahori K, Ainota T. Intrahepatic distant metastasis and metachronous multicentric occurrence in solitary hepatocellular carcinoma of less than five centimeters in diameter. Surg Today. 1993. 23:969–978.
Article13. Colombo M, de Franchis R, Del Ninno E, Sangiovanni A, De Fazio C, Tommasini M, et al. Hepatocellular carcinoma in Italian patients with cirrhosis. N Engl J Med. 1991. 325:675–680.
Article14. Tsukuma H, Hiyama T, Tanaka S, Nakao M, Yabuuchi T, Kitamura T, et al. Risk factors for hepatocellular carcinoma among patients with chronic liver disease. N Engl J Med. 1993. 328:1797–1801.
Article15. Imamura H, Matsuyama Y, Tanaka E, Ohkubo T, Hasegawa K, Miyagawa S, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003. 38:200–207.
Article16. Shirabe K, Kanematsu T, Matsumata T, Adachi E, Akazawa K, Sugimachi K. Factors linked to early recurrence of small hepatocellular carcinoma after hepatectomy: univariate and multivariate analyses. Hepatology. 1991. 14:802–805.
Article17. Lim JH, Jang HJ, Kim EY, Park CK, Joh JW, Kim YI. Early recurring hepatocellular carcinoma after partial hepatic resection: preoperative CT findings. Korean J Radiol. 2000. 1:38–42.
Article18. Shah SA, Cleary SP, Wei AC, Yang I, Taylor BR, Hemming AW, et al. Recurrence after liver resection for hepatocellular carcinoma: risk factors, treatment, and outcomes. Surgery. 2007. 141:330–339.
Article19. Park JH, Koh KC, Choi MS, Lee JH, Yoo BC, Paik SW, et al. Analysis of risk factors associated with early multinodular recurrences after hepatic resection for hepatocellular carcinoma. Am J Surg. 2006. 192:29–33.
Article20. Tanaka S, Noguchi N, Ochiai T, Kudo A, Nakamura N, Ito K, et al. Outcomes and recurrence of initially resectable hepatocellular carcinoma meeting milan criteria: Rationale for partial hepatectomy as first strategy. J Am Coll Surg. 2007. 204:1–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk Factors of Early Recurrenec after Curative Hepatic Resection for Hepatocellular Carcinoma
- The Risk Factors for Intrahepatic Early Recurrence after Resection for Hepatocellular Carcinoma
- Extrahepatic recurrence of hepatocellular carcinoma after curative hepatic resection
- Patterns of Recurrence after Curative Resection of Hepatocellular Carcinoma: Radiological Type
- Two Cases of Early Recurred Hepatocellular Carcinoma after Surgical Resection Which Showed Different Outcomes
