J Korean Med Sci.
2012 Aug;27(8):907-913. 10.3346/jkms.2012.27.8.907.
Minor Criteria of Infectious Disease Society of America/American Thoracic Society for Severe Community-Acquired Pneumonia Can Predict Delayed Treatment Response
- Affiliations
-
- 1Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Chuncheon Sacred Heart Hospital, Lung Research Institute of Hallym University, Chuncheon, Korea.
- 2Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea. pulmoks@hallym.ac.kr
- 3Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Seoul, Korea.
- KMID: 1714203
- DOI: http://doi.org/10.3346/jkms.2012.27.8.907
Abstract
- The purpose of this study was to investigate the clinical aspects of patients satisfying the Infectious Disease Society of America/American Thoracic Society (IDSA/ATS) minor severity criteria, focusing on their treatment response to empirical antibiotics. In total, 381 community-acquired pneumonia (CAP) patients who did not require mechanical ventilation or vasopressors at admission were enrolled, and 50 (13.1%) satisfied the minor severity criteria (i.e. , minor severe CAP [minor-SCAP]). The rates of new complication events and clinical treatment failure were significantly higher in the minor-SCAP group than in the control group (30.0% vs 2.1%, P < 0.001, and 42.0% vs 10.6%, P < 0.001, respectively), and the time to reach clinical stability was longer in the minor-SCAP group (8 days vs 3 days, P < 0.001). In a multivariate model, minor severity criteria (> or = 3) were significantly associated with treatment failure (odds ratio, 2.838; 95% confidence interval, 1.216 to 6.626), and for predicting treatment failure the value of the area under the receiver operating characteristic curve for minor criteria was 0.731, similar to other established scoring methods. The IDSA/ATS minor severity criteria can predict delayed treatment response and clinical treatment failure.
Keyword
MeSH Terms
-
Adult
Aged
Anti-Bacterial Agents/therapeutic use
Area Under Curve
Community-Acquired Infections/*diagnosis/drug therapy/mortality
Female
Hospital Mortality
Humans
Intensive Care Units
Kaplan-Meier Estimate
Length of Stay
Male
Middle Aged
Odds Ratio
Pneumonia/*diagnosis/drug therapy/mortality
Predictive Value of Tests
ROC Curve
*Severity of Illness Index
Anti-Bacterial Agents
Figure
-
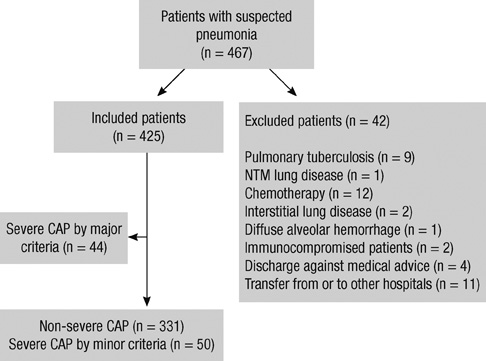
Fig. 1 Flowchart of the patient population. CAP, community-acquired pneumonia; ICU, intensive care unit; NTM, nontuberculous mycobacteria.

Fig. 2 Kaplan-Meier survival curves for the time to reach clinical stability. The time to reach clinical stability was longer in the minor-SCAP than in the control (i.e., non-SCAP) groups (log rank = 28.6, P < 0.001).
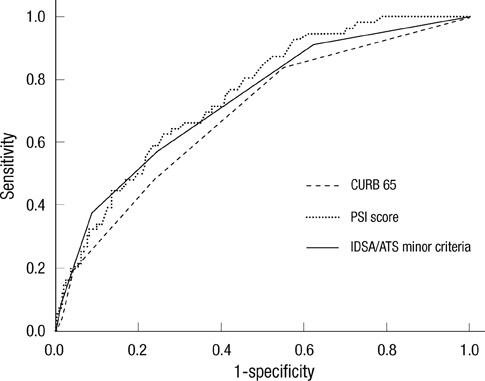
Fig. 3 ROC curves for prediction of clinical treatment failure. The AUC values for the minor criteria, CURB-65 and PSI scores were 0.731 (95% CI, 0.660-0.802), 0.688 (95% CI, 0.614-0.762), and 0.751 (95% CI, 0.688-0.814), respectively.
Reference
-
1. Hoogewerf M, Oosterheert JJ, Hak E, Hoepelman IM, Bonten MJ. Prognostic factors for early clinical failure in patients with severe community-acquired pneumonia. Clin Microbiol Infect. 2006. 12:1097–1104.2. Menendez R, Torres A, Zalacain R, Aspa J, Martin Villasclaras JJ, Borderias L, Benitez Moya JM, Ruiz-Manzano J, Rodriguez de Castro F, Blanquer J, et al. Risk factors of treatment failure in community acquired pneumonia: implications for disease outcome. Thorax. 2004. 59:960–965.3. Restrepo MI, Mortensen EM, Velez JA, Frei C, Anzueto A. A comparative study of community-acquired pneumonia patients admitted to the ward and the ICU. Chest. 2008. 133:610–617.4. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM Jr, Musher DM, Niederman MS, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007. 44:S27–S72.5. Liapikou A, Ferrer M, Polverino E, Balasso V, Esperatti M, Piner R, Mensa J, Luque N, Ewig S, Menendez R, et al. Severe community-acquired pneumonia: validation of the Infectious Diseases Society of America/American Thoracic Society guidelines to predict an intensive care unit admission. Clin Infect Dis. 2009. 48:377–385.6. Phua J, See KC, Chan YH, Widjaja LS, Aung NW, Ngerng WJ, Lim TK. Validation and clinical implications of the IDSA/ATS minor criteria for severe community-acquired pneumonia. Thorax. 2009. 64:598–603.7. Chalmers JD, Taylor JK, Mandal P, Choudhury G, Singanayagam A, Akram AR, Hill AT. Validation of the Infectious Diseases Society of America/American Thoratic Society minor criteria for intensive care unit admission in community-acquired pneumonia patients without major criteria or contraindications to intensive care unit care. Clin Infect Dis. 2011. 53:503–511.8. Hilbert G, Gruson D, Vargas F, Valentino R, Gbikpi-Benissan G, Dupon M, Reiffers J, Cardinaud JP. Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure. N Engl J Med. 2001. 344:481–487.9. Siegel RE. Time to clinical stability for patients with community-acquired pneumonia. JAMA. 1999. 281:231–232.10. Menendez R, Torres A, Rodriguez de Castro F, Zalacain R, Aspa J, Martin Villasclaras JJ, Borderias L, BenitezMoya JM, Ruiz-Manzano J, Blanquer J, et al. Reaching stability in community-acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004. 39:1783–1790.11. Lim WS, van der Eerden MM, Laing R, Boersma WG, Karalus N, Town GI, Lewis SA, Macfarlane JT. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003. 58:377–382.12. Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, Coley CM, Marrie TJ, Kapoor WN. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997. 336:243–250.13. Menendez R, Torres A. Treatment failure in community-acquired pneumonia. Chest. 2007. 132:1348–1355.14. Espana PP, Capelastegui A, Gorordo I, Esteban C, Oribe M, Ortega M, Bilbao A, Quintana JM. Development and validation of a clinical prediction rule for severe community-acquired pneumonia. Am J Respir Crit Care Med. 2006. 174:1249–1256.15. Levin KP, Hanusa BH, Rotondi A, Singer DE, Coley CM, Marrie TJ, Kapoor WN, Fine MJ. Arterial blood gas and pulse oximetry in initial management of patients with community-acquired pneumonia. J Gen Intern Med. 2001. 16:590–598.16. Blot SI, Rodriguez A, Sole-Violan J, Blanquer J, Almirall J, Rello J. Effects of delayed oxygenation assessment on time to antibiotic delivery and mortality in patients with severe community-acquired pneumonia. Crit Care Med. 2007. 35:2509–2514.17. Yandiola PP, Capelastegui A, Quintana J, Diez R, Gorordo I, Bilbao A, Zalacain R, Menendez R, Torres A. Prospective comparison of severity scores for predicting clinically relevant outcomes for patients hospitalized with community-acquired pneumonia. Chest. 2009. 135:1572–1579.18. Guo Q, Li HY, Zhou YP, Li M, Chen XK, Liu H, Peng HL, Yu HQ, Chen X, Liu N, et al. Weight of the IDSA/ATS minor criteria for severe community-acquired pneumonia. Respir Med. 2011. 105:1543–1549.19. Brown SM, Jones BE, Jephson AR, Dean NC. Validation of the Infectious Disease Society of America/American Thoracic Society 2007 guidelines for severe community-acquired pneumonia. Crit Care Med. 2009. 37:3010–3016.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Respiratory Review of 2010: Pneumonia
- Community-acquired pneumonia in elderly patients
- Patient Stratification and Decision to Hospitalize Patients with Community-Acquired Pneumonia
- Community Acquired Pneumonia
- Treatment Guidelines for Community-acquired Pneumonia in Korea: An Evidence-based Approach to Appropriate Antimicrobial Therapy
