Multidetector Computed Tomography for the Assessment of Adnexal Mass: Is Unenhanced CT Scan Necessary?
- Affiliations
-
- 1Department of Radiology, Research Institute of Medical Science, Konkuk University School of Medicine, Seoul 143-729, Korea. radsijung@kuh.ac.kr
- KMID: 1711480
- DOI: http://doi.org/10.3348/kjr.2014.15.1.72
Abstract
OBJECTIVE
To compare the diagnostic performance and radiation dose between contrast-enhanced CT (ECT) alone, and combined unenhanced and contrast-enhanced CT (UE + ECT) for the assessment of adnexal mass.
MATERIALS AND METHODS
This retrospective study was approved by the Institutional Review Board. A total of 146 consecutive patients (mean age, 41.1 years) who underwent preoperative unenhanced and contrast-enhanced multidetector CT of the pelvis and had adnexal masses found at surgery were included. Two readers independently evaluated the likelihood of adnexal malignancy on a 5-point scale on two different imaging datasets (ECT alone and UE + ECT). The area under the receiver operating characteristic curve (AUC) was used to evaluate diagnostic performance. Radiation dose to patients was calculated by the volume CT dose index (CTDIvol) and the dose length products (DLP) on each dataset.
RESULTS
Of the total 178 adnexal masses, 133 masses were benign and 45 masses were malignant. For both readers, there is no significant difference of AUC values between ECT alone and UE + ECT for the detection of adnexal malignancy (reader 1, 0.93 vs. 0.95; reader 2, 0.92 vs. 0.91) (p > 0.05). The mean CTDIvol (12.6 +/- 2.2 mGy) and DLP (641.2 +/- 137.2 mGy) of ECT alone was significantly lower than the mean CTDIvol (21.5 +/- 2.7 mGy) and DLP (923.6 +/- 158.8 mGy) of UE + ECT (p < 0.0001).
CONCLUSION
The use of unenhanced CT scan in addition to contrast-enhanced CT scan does not improve the detection of adnexal malignancy, but increases radiation exposure.
Keyword
MeSH Terms
Figure
-
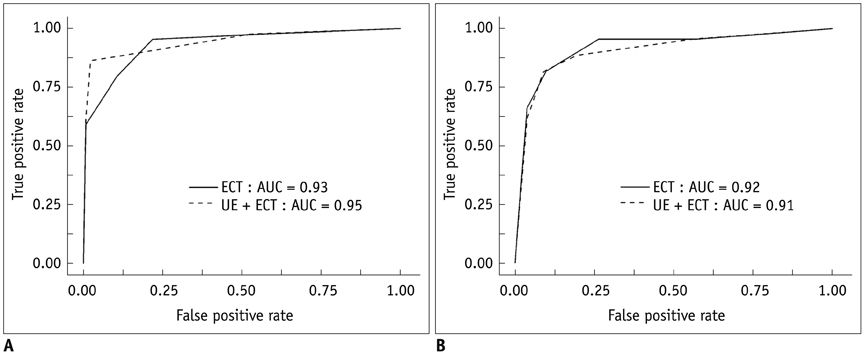
Fig. 1 Receiver operating characteristic curve for readers 1 (A) and 2 (B) for detection of adnexal malignancy on ECT images alone and UE + ECT images. ECT = enhanced CT, UE + ECT = combined unenhanced and enhanced CT
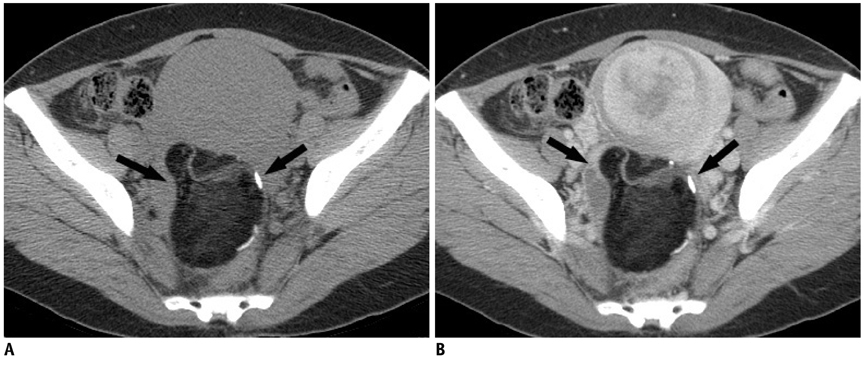
Fig. 2 46-year-old woman with complaint of pelvic mass. Unenhanced CT scan (A) and contrast-enhanced CT scan (B) show large fatty mass with calcification (arrows) in pelvic cavity. Likelihood of malignancy was assigned score 1 (definitely benign) to this adnexal mass both on ECT images alone and UE + ECT images. Surgical pathology confirmed right ovarian teratoma. ECT = enhanced CT, UE + ECT = combined unenhanced and enhanced CT

Fig. 3 54-year-old woman with complaint of pelvic mass. Unenhanced CT scan (A) and contrast-enhanced CT scan (B) shows multilocular cystic mass with well-enhanced sold component (arrow) in pelvic cavity. Likelihood of malignancy was assigned score of 5 (definitely malignant) to this adnexal mass, both on ECT images alone and UE + ECT images. Surgical pathology confirmed endometrioid adenocarcinoma of right ovary. ECT = enhanced CT, UE + ECT = combined unenhanced and enhanced CT
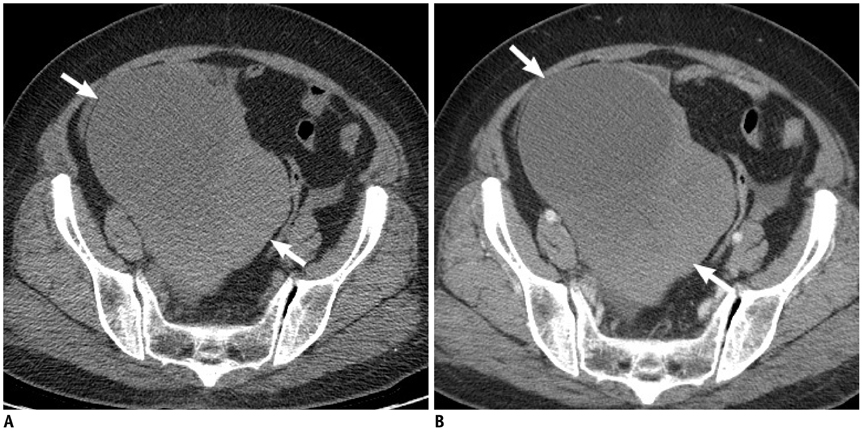
Fig. 4 63-year-old woman with complaint of pelvic mass. Unenhanced CT scan (A) and contrast-enhanced CT scan (B) show large complex mass containing both cyst and solid components in right pelvic cavity (arrows). Solid component seems to be homogeneous and lacking in contrast-enhancement. Likelihood of malignancy was assigned score of 3 (intermediate) to this adnexal mass on ECT images alone, and score of 2 (probably benign) on UE + ECT images. Surgical pathology confirmed right ovarian fibroma. ECT = enhanced CT, UE + ECT = combined unenhanced and enhanced CT

Fig. 5 49-year-old woman with complaint of pelvic mass. Unenhanced CT scan (A) and contrast-enhanced CT scan (B) shows large multilocular cystic mass with solid component in left pelvic cavity (arrows). Solid component has high attenuation on unenhanced CT scan (arrowheads). Likelihood of malignancy was assigned score of 4 (probably malignant) to this adnexal mass on ECT images alone, and score of 3 (intermediate) on UE + ECT images. Surgical pathology confirmed mucinous borderline tumor of left ovary. ECT = enhanced CT, UE + ECT = combined unenhanced and enhanced CT
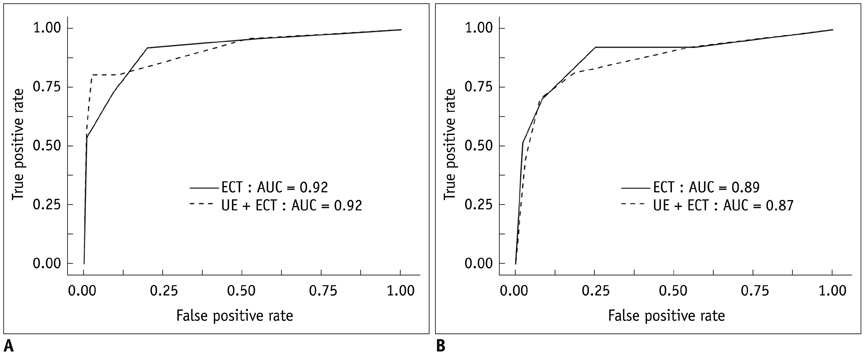
Fig. 6 Receiver operating characteristic curve for readers (A) 1 and (B) 2 for detection of adnexal malignancy without ancillary findings on ECT images alone and UE + ECT images. ECT = enhanced CT, UE + ECT = combined unenhanced and enhanced CT
Reference
-
1. Salem S, White LM, Lai J. Doppler sonography of adnexal masses: the predictive value of the pulsatility index in benign and malignant disease. AJR Am J Roentgenol. 1994; 163:1147–1150.2. Spencer JA, Ghattamaneni S. MR imaging of the sonographically indeterminate adnexal mass. Radiology. 2010; 256:677–694.3. Hricak H, Chen M, Coakley FV, Kinkel K, Yu KK, Sica G, et al. Complex adnexal masses: detection and characterization with MR imaging--multivariate analysis. Radiology. 2000; 214:39–46.4. Tsili AC, Tsampoulas C, Charisiadi A, Kalef-Ezra J, Dousias V, Paraskevaidis E, et al. Adnexal masses: accuracy of detection and differentiation with multidetector computed tomography. Gynecol Oncol. 2008; 110:22–31.5. Zhang J, Mironov S, Hricak H, Ishill NM, Moskowitz CS, Soslow RA, et al. Characterization of adnexal masses using feature analysis at contrast-enhanced helical computed tomography. J Comput Assist Tomogr. 2008; 32:533–540.6. Tsili AC, Tsampoulas C, Argyropoulou M, Navrozoglou I, Alamanos Y, Paraskevaidis E, et al. Comparative evaluation of multidetector CT and MR imaging in the differentiation of adnexal masses. Eur Radiol. 2008; 18:1049–1057.7. Greess H, Nömayr A, Wolf H, Baum U, Lell M, Böwing B, et al. Dose reduction in CT examination of children by an attenuation-based on-line modulation of tube current (CARE Dose). Eur Radiol. 2002; 12:1571–1576.8. Tack D, De Maertelaer V, Gevenois PA. Dose reduction in multidetector CT using attenuation-based online tube current modulation. AJR Am J Roentgenol. 2003; 181:331–334.9. Paterson A, Frush DP, Donnelly LF. Helical CT of the body: are settings adjusted for pediatric patients? AJR Am J Roentgenol. 2001; 176:297–301.10. Divrik Gökçe S, Gökçe E, Coşkun M. Radiology residents' awareness about ionizing radiation doses in imaging studies and their cancer risk during radiological examinations. Korean J Radiol. 2012; 13:202–209.11. Goo HW. CT radiation dose optimization and estimation: an update for radiologists. Korean J Radiol. 2012; 13:1–11.12. Hur S, Lee JM, Kim SJ, Park JH, Han JK, Choi BI. 80-kVp CT using Iterative Reconstruction in Image Space algorithm for the detection of hypervascular hepatocellular carcinoma: phantom and initial clinical experience. Korean J Radiol. 2012; 13:152–164.13. Moritz JD, Hoffmann B, Sehr D, Keil K, Eggerking J, Groth G, et al. Evaluation of ultra-low dose CT in the diagnosis of pediatric-like fractures using an experimental animal study. Korean J Radiol. 2012; 13:165–173.14. Park EA, Lee W, Kang JH, Yin YH, Chung JW, Park JH. The image quality and radiation dose of 100-kVp versus 120-kVp ECG-gated 16-slice CT coronary angiography. Korean J Radiol. 2009; 10:235–243.15. Stevens SK, Hricak H, Stern JL. Ovarian lesions: detection and characterization with gadolinium-enhanced MR imaging at 1.5 T. Radiology. 1991; 181:481–488.16. Obuchowski NA. Nonparametric analysis of clustered ROC curve data. Biometrics. 1997; 53:567–578.17. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33:159–174.18. Togashi K. Ovarian cancer: the clinical role of US, CT, and MRI. Eur Radiol. 2003; 13:Suppl 4. L87–L104.19. Liu J, Xu Y, Wang J. Ultrasonography, computed tomography and magnetic resonance imaging for diagnosis of ovarian carcinoma. Eur J Radiol. 2007; 62:328–334.20. O'Malley ME, Halpern E, Mueller PR, Gazelle GS. Helical CT protocols for the abdomen and pelvis: a survey. AJR Am J Roentgenol. 2000; 175:109–113.21. Killius JS, Nelson RC. Logistic advantages of four-section helical CT in the abdomen and pelvis. Abdom Imaging. 2000; 25:643–650.22. Urban BA, Fishman EK. Tailored helical CT evaluation of acute abdomen. Radiographics. 2000; 20:725–749.23. Johnstone PA. ACR appropriateness criteria. Int J Radiat Oncol Biol Phys. 2008; 70:1303–1304.24. Gatreh-Samani F, Tarzamni MK, Olad-Sahebmadarek E, Dastranj A, Afrough A. Accuracy of 64-multidetector computed tomography in diagnosis of adnexal tumors. J Ovarian Res. 2011; 4:15.25. Tsushima Y, Yamada S, Aoki J, Motojima T, Endo K. Effect of contrast-enhanced computed tomography on diagnosis and management of acute abdomen in adults. Clin Radiol. 2002; 57:507–513.26. Guite KM, Hinshaw JL, Ranallo FN, Lindstrom MJ, Lee FT Jr. Ionizing radiation in abdominal CT: unindicated multiphase scans are an important source of medically unnecessary exposure. J Am Coll Radiol. 2011; 8:756–761.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Added Value of Using a CT Coronal Reformation to Diagnose Adnexal Torsion
- Periureteral Varices with Accompanying Pyelitis Diagnosed by 3-Dimensional Reformatted Technique of the Multidetector Row CT: A Case Report
- Follicular Dendritic Cell Sarcoma of the Omentum: Multidetector Computed Tomography Findings
- MDCT Application of Thoracic Imaging
- Multidetector Row Computed Tomography: 'Principles and Clinical Applications'
