Added Value of Using a CT Coronal Reformation to Diagnose Adnexal Torsion
- Affiliations
-
- 1Department of Radiology, Konkuk University School of Medicine, Research Institute of Medical Science, Seoul 143-729, Korea.
- 2Department of Obstetrics and Gynecology, School of Medicine, Ewha Womans University, Seoul 158-710, Korea. ogjeong@ewha.ac.kr
- KMID: 2155557
- DOI: http://doi.org/10.3348/kjr.2015.16.4.835
Abstract
OBJECTIVE
To evaluate the increased value of using coronal reformation of a transverse computed tomography (CT) scan for detecting adnexal torsion.
MATERIALS AND METHODS
This study included 106 woman suspected of having adnexal torsion who underwent CT with coronal reformations and subsequent surgical exploration. Two readers independently recorded the CT findings, such as the thickening of a fallopian tube, twisting of the adnexal pedicle, eccentric smooth wall thickening of the torsed adnexal mass, eccentric septal thickening of the torsed adnexal mass, eccentric poor enhancement of the torsed adnexal mass, uterine deviation to the twisted side, ascites or infiltration of pelvic fat, and the overall impression of adnexal torsion with a transverse scan alone or combined with coronal reformation and a transverse scan. The areas under the receiver operating characteristic curves (AUCs), sensitivity, specificity, and positive predictive value were used to compare diagnostic performance.
RESULTS
Fifty-two patients were confirmed to have adnexal torsion. The addition of coronal reformations to the transverse scan improved AUCs for readers 1 and 2 from 0.74 and 0.75 to 0.92 and 0.87, respectively, for detecting adnexal torsion (p < 0.001 and p = 0.004, respectively). Sensitivity of CT for detecting twisting of the adnexal pedicle increased significantly for readers 1 and 2 from 0.27 and 0.29 with a transverse scan alone to 0.79 and 0.77 with a combined coronal reformation and a transverse scan, respectively (p < 0.001 and p < 0.001, respectively).
CONCLUSION
Use of a coronal reformation with transverse CT images improves detection of adnexal torsion.
MeSH Terms
-
Acute Pain/diagnosis/radiography
Adnexa Uteri/pathology/*radiography
Adnexal Diseases/*radiography
Adolescent
Adult
Aged
Aged, 80 and over
Area Under Curve
Child
Female
Humans
Middle Aged
Pelvis/radiography
ROC Curve
Retrospective Studies
Tomography, X-Ray Computed/*methods
Torsion Abnormality/*diagnosis/*radiography
Young Adult
Figure
-
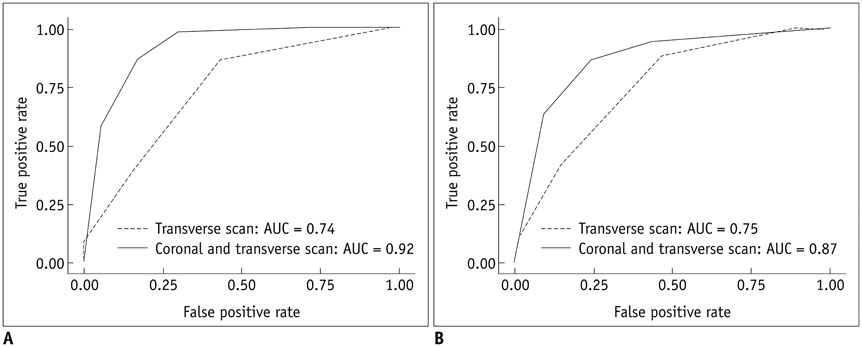
Fig. 1 Receiver operating characteristic curves for reader 1 (A) and reader 2 (B) for detecting adnexal torsion. AUC = areas under receiver operating characteristic curve

Fig. 2 Contrast-enhanced computed tomography (CT) scan of 66-year-old woman with torsion of follicular cyst in right ovary. Transverse CT scan (A) and coronal reformation (B) show multilocular cystic mass with homogeneously elongated soft tissue lesion representing tubal thickening (arrows).
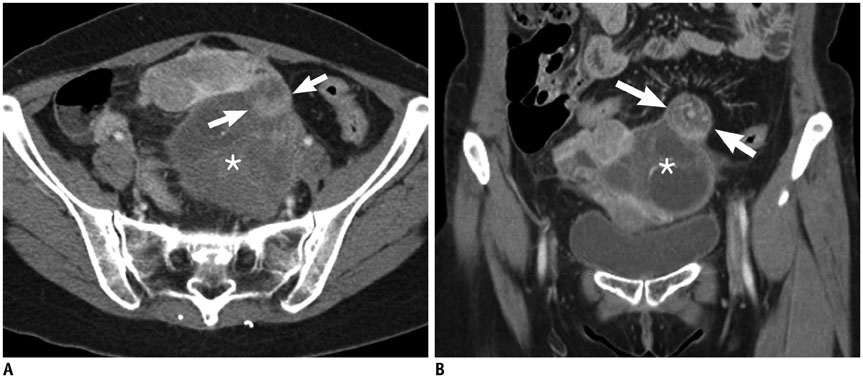
Fig. 3 Contrast-enhanced computed tomography (CT) scan of 53-year-old woman with torsion of follicular cyst in left ovary. Transverse CT scan (A) and coronal reformation (B) show heterogeneous cystic mass (*) with swirling soft tissue lesion representing twisting of adnexal pedicle (arrows).

Fig. 4 Contrast-enhanced computed tomography (CT) scan of 41-year-old woman with torsion of follicular cyst in right ovary. Transverse CT scan (A) and coronal reformation (B) show unilocular cystic mass with eccentric smooth wall thickening (arrows).

Fig. 5 Contrast-enhanced computed tomography (CT) scan of 52-year-old woman with torsion of follicular cyst in right ovary. Transverse CT scan (A) and coronal reformation (B) show eccentric septal thickening (arrow) of cystic mass.

Fig. 6 Contrast-enhanced computed tomography (CT) scan of 49-year-old woman with complaint of acute pelvic pain as false-negative case. Transverse CT scan (A) and coronal reformation (B) show well-defined cystic mass (*) in pelvic cavity. Both readers provided scores of 2 as level of suspicion for adnexal torsion using 5-point scale. Adnexal mass was serous cystadenoma with torsion in right ovary.
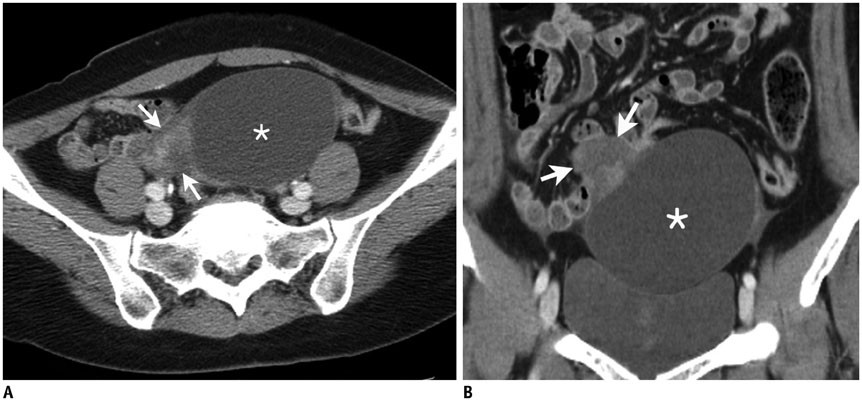
Fig. 7 Contrast-enhanced computed tomography (CT) scan in 38-year-old woman with complaint of acute pelvic pain as false-positive case. Transverse CT scan (A) and coronal reformation (B) show well-defined cystic mass (*) with eccentric soft tissue lesion (arrows). Both readers provided score of 4 as level of suspicion for adnexal torsion using 5-point scale. Adnexal mass was paratubal cyst without torsion in right ovary.
Reference
-
1. Chiou SY, Lev-Toaff AS, Masuda E, Feld RI, Bergin D. Adnexal torsion: new clinical and imaging observations by sonography, computed tomography, and magnetic resonance imaging. J Ultrasound Med. 2007; 26:1289–1301.2. Hiller N, Appelbaum L, Simanovsky N, Lev-Sagi A, Aharoni D, Sella T. CT features of adnexal torsion. AJR Am J Roentgenol. 2007; 189:124–129.3. Kiechl-Kohlendorfer U, Maurer K, Unsinn KM, Gassner I. Fluid-debris level in follicular cysts: a pathognomonic sign of ovarian torsion. Pediatr Radiol. 2006; 36:421–425.4. Albayram F, Hamper UM. Ovarian and adnexal torsion: spectrum of sonographic findings with pathologic correlation. J Ultrasound Med. 2001; 20:1083–1089.5. Auslender R, Shen O, Kaufman Y, Goldberg Y, Bardicef M, Lissak A, et al. Doppler and gray-scale sonographic classification of adnexal torsion. Ultrasound Obstet Gynecol. 2009; 34:208–211.6. Graif M, Shalev J, Strauss S, Engelberg S, Mashiach S, Itzchak Y. Torsion of the ovary: sonographic features. AJR Am J Roentgenol. 1984; 143:1331–1334.7. Rha SE, Byun JY, Jung SE, Jung JI, Choi BG, Kim BS, et al. CT and MR imaging features of adnexal torsion. Radiographics. 2002; 22:283–294.8. Rosado WM Jr, Trambert MA, Gosink BB, Pretorius DH. Adnexal torsion: diagnosis by using Doppler sonography. AJR Am J Roentgenol. 1992; 159:1251–1253.9. Boone JM. Multidetector CT: opportunities, challenges, and concerns associated with scanners with 64 or more detector rows. Radiology. 2006; 241:334–337.10. Jaffe TA, Nelson RC, Johnson GA, Lee ER, Yoshizumi TT, Lowry CR, et al. Optimization of multiplanar reformations from isotropic data sets acquired with 16-detector row helical CT scanner. Radiology. 2006; 238:292–299.11. Hodel J, Zins M, Desmottes L, Boulay-Coletta I, Jullès MC, Nakache JP, et al. Location of the transition zone in CT of small-bowel obstruction: added value of multiplanar reformations. Abdom Imaging. 2009; 34:35–41.12. Jaffe TA, Martin LC, Thomas J, Adamson AR, DeLong DM, Paulson EK. Small-bowel obstruction: coronal reformations from isotropic voxels at 16-section multi-detector row CT. Radiology. 2006; 238:135–142.13. Noroozian M, Cohan RH, Caoili EM, Cowan NC, Ellis JH. Multislice CT urography: state of the art. Br J Radiol. 2004; 77 Spec No 1:S74–S86.14. Paulson EK, Harris JP, Jaffe TA, Haugan PA, Nelson RC. Acute appendicitis: added diagnostic value of coronal reformations from isotropic voxels at multi-detector row CT. Radiology. 2005; 235:879–885.15. Duigenan S, Oliva E, Lee SI. Ovarian torsion: diagnostic features on CT and MRI with pathologic correlation. AJR Am J Roentgenol. 2012; 198:W122–W131.16. Lee JH, Park SB, Shin SH, Jang JC, Lee WC, Jeong AK, et al. Value of intra-adnexal and extra-adnexal computed tomographic imaging features diagnosing torsion of adnexal tumor. J Comput Assist Tomogr. 2009; 33:872–876.17. Dunnihoo DR, Wolff J. Bilateral torsion of the adnexa: a case report and a review of the world literature. Obstet Gynecol. 1984; 64:3 Suppl. 55S–59S.18. Song HH. Analysis of correlated ROC areas in diagnostic testing. Biometrics. 1997; 53:370–382.19. Molodianovitch K, Faraggi D, Reiser B. Comparing the areas under two correlated ROC curves: parametric and non-parametric approaches. Biom J. 2006; 48:745–757.20. Cohen J. Weighted kappa: nominal scale agreement with provision for scaled disagreement or partial credit. Psychol Bull. 1968; 70:213–220.21. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33:159–174.22. Shadinger LL, Andreotti RF, Kurian RL. Preoperative sonographic and clinical characteristics as predictors of ovarian torsion. J Ultrasound Med. 2008; 27:7–13.23. Warner MA, Fleischer AC, Edell SL, Thieme GA, Bundy AL, Kurtz AB, et al. Uterine adnexal torsion: sonographic findings. Radiology. 1985; 154:773–775.24. Lee EJ, Kwon HC, Joo HJ, Suh JH, Fleischer AC. Diagnosis of ovarian torsion with color Doppler sonography: depiction of twisted vascular pedicle. J Ultrasound Med. 1998; 17:83–89.25. Vijayaraghavan SB. Sonographic whirlpool sign in ovarian torsion. J Ultrasound Med. 2004; 23:1643–1649. quiz 1650-165126. Chang HC, Bhatt S, Dogra VS. Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics. 2008; 28:1355–1368.27. Comerci JT Jr, Licciardi F, Bergh PA, Gregori C, Breen JL. Mature cystic teratoma: a clinicopathologic evaluation of 517 cases and review of the literature. Obstet Gynecol. 1994; 84:22–28.28. Paulson EK, Jaffe TA, Thomas J, Harris JP, Nelson RC. MDCT of patients with acute abdominal pain: a new perspective using coronal reformations from submillimeter isotropic voxels. AJR Am J Roentgenol. 2004; 183:899–906.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of torsion of normal adenexa misdiagnosed as left inguinal hernia in a neonate
- A case of torsion of an omental leiomyoma misdiagnosed as torsion of an adnexal mass
- Isolated Torsion of Fallopian Tubes: Detection of Pedicle at Tubal End: Two Case Report
- A case of Adnexal Torsion in Pregnancy
- The Benefit of Added Coronal Reformation Images in the MDCT Diagnosis of Acute Appendicitis for Emergency Physicians
