A Case of Parathyroid Adenoma Manifested as Acute Pancreatitis Accompanied Subclinical Cushing's Syndrome due to an Adrenal Adenoma
- Affiliations
-
- 1Department of Internal Medicine, Seoul Adventist Hospital.
- 2Department of Anatomical Pathology, Seoul Adventist Hospital.
- KMID: 1523105
- DOI: http://doi.org/10.3803/jkes.2007.22.5.353
Abstract
- The manifestation of primary hyperparathyroidism by acute pancreatitis is a rare event. Furthermore, an asymptomatic adrenal mass may incidentally be detected by abdominal computed tomography. A mass that autonomously secretes glucocorticoid without any symptom is called subclinical Cushing's syndrome. In this study, we report a rare case of a parathyroid adenoma manifested as acute pancreatitis accompanied with subclinical Cushing's syndrome due to an incidental adrenal mass. A 47-year-old female patient presented with acute pancreatitis and hypercalcemia had a parathyroid mass detected by neck ultrasonography and a Tc(99m)-sestamibi scan. An abdominal computed tomography revealed a 3.1 x 4.3 cm mass which was detected in the left adrenal gland. The hormonal levels showed a high serum cortisol level, low ACTH level, and a high 24 h urine free cortisol level. The low and high dose dexamethasone suppression test showed no suppression. The parathyroid and adrenal masses were resected and the laboratory findings were normalized.
MeSH Terms
Figure
-

Figure 1 Tc99m-sestamibi scan shows increased uptake in the right parathyroid region.
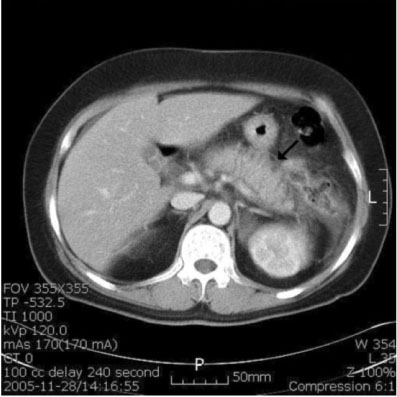
Figure 2 Abdomen CT demonstrates edematous pancreas with peripancreatic fluid collection.

Figure 3 Abdomen CT scan demonstrates left adrenal mass which is about 3.1 × 4.3 cm sized, well-marginated & homogeneous soft-tissue mass.

Figure 4 Abdominal CT scan demonstrates about 3.2 cm sized, well-marginated & round soft-tissue mass in left side of cul-de-sac, normal uterus & ovaries.
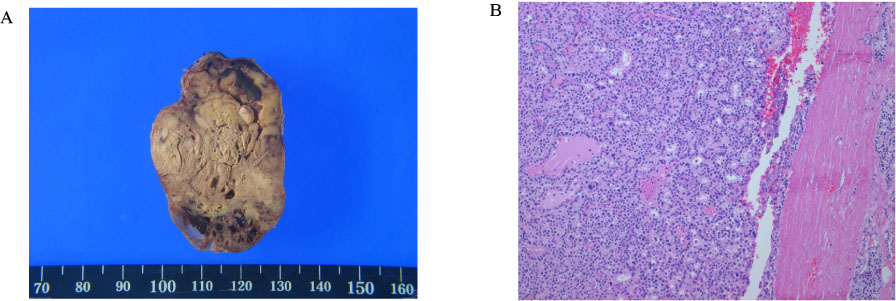
Figure 5 (A) Gross appearance of the parathyroid adenoma. (B) Microscopic finding of the parathyroid adenoma. Parathyroid adenoma is composed of solid sheet-like, acinar, follicle-like arrangement of parathyroid chief cells. There are normal parathyroidal glands within the fibrous capsular stroma (H & E stain, ×100).

Figure 6 (A) Gross appearance of the adrenal mass. (B) Microscopic finding of the adrenal adenoma. Adrenal adenoma reveals solid nests or cords of cells with pale abundant cytoplasm (H & E stain, ×40).
Reference
-
1. McMahon A. Parathyroidism. Tr AM Therap Soc. 1934. 34:176–178.2. Cope O, Culver PJ, Mixter CG, Nardi GL. Pancreatitis as a diagnostic clue to hyper-parathyroidism. Ann Surg. 1957. 145:857–863.3. Fink WJ, Finfrock JD. Fatal hyperparathyroid crisis associated with pancreatitis. Am Surgery. 1961. 27:424–430.4. Kwon YK, Lee MM, Yu SH, Kang HS, Kim SW, Yang IM, Kim JW, Kim YS, Kim KW, Choi YK. A case of parathyroid adenoma associated with acute pancreatitis as a initial manifestation. J Kor Soc Endocrinol. 1990. 5:141–144.5. Lee BJ, Won YJ, Song YD, Lim SK, Kim JM, Lee HC, Lee YB, Huh KB. Two cases of hyperparathyroidism presenting as acute pancreatitis. J Kor Soc Endocrinol. 1997. 12:321–327.6. Young WF Jr. Clinical practice. The incidentally discovered adrenal mass. N Engl J Med. 2007. 356:601–610.7. Adami S, Marcocci C, Gatti D. Epidemiology of primary hyperparathyroidism in Europe. J Bone Miner Res. 2002. 17:18–23.8. Mixter CG, Keynes WM, Cope O. Further experience with pancreatitis as a diagnostic clue to hyperparathyroidism. N Eng J Med. 1962. 266:265–272.9. Bess MA, Edis AJ, van Heerden JA. Hyper- parathyroidism & pancreatitis. chance or a causal association? JAMA. 1980. 243:246–247.10. Koppelberg T, Bartsch D, Printz H, Hasse C, Rothmund M. Pancreatitis in prim ary hyperparathyroidism(pHPT) is a complication of advanced pHPT. Dtsch Med Wochenschr. 1994. 119:719–724.11. Agarwal A, George RK, Gupta SK, Mishra SK. Pancreatitis in patients w ith prim ary hyperparathyroidism. Indian J Gastroenterol. 2003. 22:224–225.12. Layer P, Hotz J, Schmitz-Moormann HP, Goebell H. Effect of experimental chronic hypercalcemia on feline exocrine pancreatic secretion. Gastroenterolgy. 1982. 82:309–316.13. Haverback BJ, Dyce B, Bundy H, Edmondson HA. Trypsin, trypsinogen and trypsin inhibitor in human pancreatic juice: mechanism for pancreatitis associated with hyperparathyroidism. AM J Med. 1960. 29:421–433.14. Halangk W, Lerch MM. Early events in acute pancreatitis. Gastroenterol Clin North Am. 2004. 33:717–731.15. Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology. 2001. 120:682–707.16. Bockus HL. Recent experience in the diagnosis and treatment of acute pancreatitis. Postgrad Gastroenterol. 1950. Philadelphia: WB Saunders.17. Reincke M. Subclinical Cushing's syndrome. Endocrinol Metab Clin North Am. 2000. 29:43–56.18. Charbonnel B, Chatal JF, Ozanne P. Does the corticoadrenal adenoma with "pre-Cushing's syndrome" exist? J Nucl Med. 1981. 22:1059–1061.19. Makino S, Oda S, Saka T, Yasukawa M, Komatsu F, Sasano H. A case of aldosterone-producing adrenocortical adenoma associated with preclinical Cushing's syndrome and hypersecretion of parathyroid hormone. Endocr J. 2001. 48:103–111.20. Sawano S, Shishiba Y, Shimizu T, Ozawa Y, Miyata E, Nakazawa H, Suzuki N, Akiyama H. Hyperparathyroidism associated with Cushing's syndrome due to an Adrenal cortical adenoma. Endocrinol Jpn. 1990. 37:255–260.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Black Adenoma of the Adrenal Cortex Associated with Cushing's Syndrome
- A Case of Bilateral ACTH-independent Adrenal Adenomas with Cushing's Syndrome Treated by Ipsilateral Total and Contralateral Partial Laparoscopic Adrenalectomy
- A Case of Parathyroid Adenoma Manifested by Acute Recurrent Pancreatitis
- A case of adrenocortical adenoma with primary hyperaldosteronism and subclinical Cushing's syndrome
- A Case of Adrenocortical Adenoma Causing Subclinical Cushing's Syndrome Mistaken for Liddle's Syndrome
