A Case of Large Left Atrial Myxoma Presenting as Atrial Flutter
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kosin University Gospel Hospital, Busan, Korea. libaek@gmail.com
- 2Department of Cardiovascular Surgery, Kosin University Gospel Hospital, Busan, Korea.
- KMID: 1491043
- DOI: http://doi.org/10.4250/jcu.2008.16.2.59
Abstract
- Cardiac myxoma is the most common benign cardiac tumor and it presents various clinical symptoms and signs. Although two-thirds of patients have abnormal electrocardiographic findings, atrial flutter or conduction abnormalities are known to be rare. We report on a case of a large left atrial myxoma which was diagnosed by trans-thoracic, trans-esophageal echocardiography, chest computerized tomography, and histological examination. The myxoma was presented as atrial flutter in a 41-year old man who was complaining palpitation and dyspnea on exertion. After surgical excision of the mass, atrial flutter converted to normal sinus rhythm. We report this case with review of literatures on left atrial myxoma associated with arrhythmia.
Keyword
MeSH Terms
Figure
-
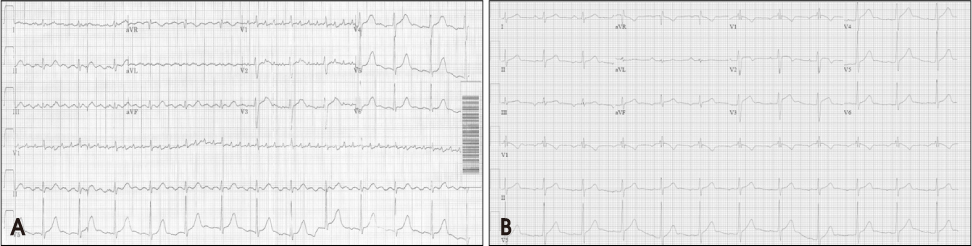
Fig. 1 Initial ECG showed atrial flutter with 4:1 AV block (A). Postoperative ECG showed normal sinus rhythm (B).
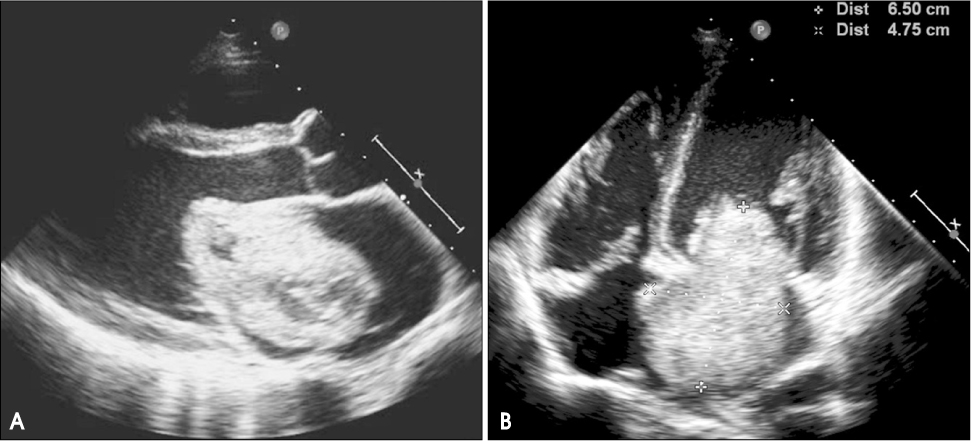
Fig. 2 Trans-throracic echocardiography showed a large mobile round mass in the left atrium with central necrosis (A and B).
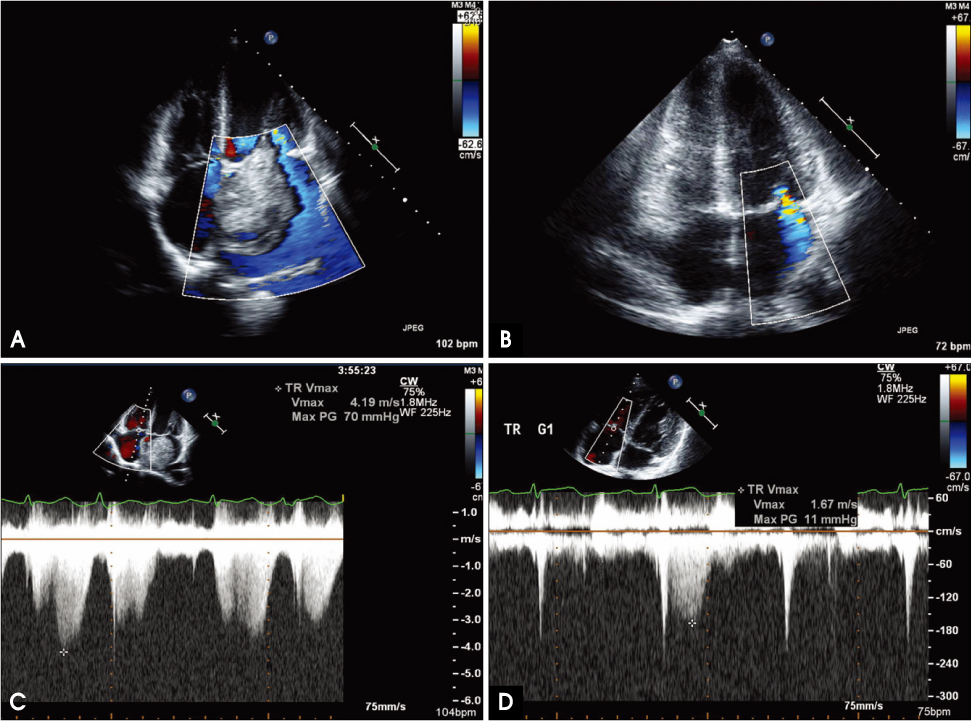
Fig. 3 Hemodynamic change on echocardiographic examination. Severe mitral regurgitation decreased after surgery (A and B). Also peak velocity of tricuspid regurgitation decreased from 4.19 to 1.67 m/s (C and D).
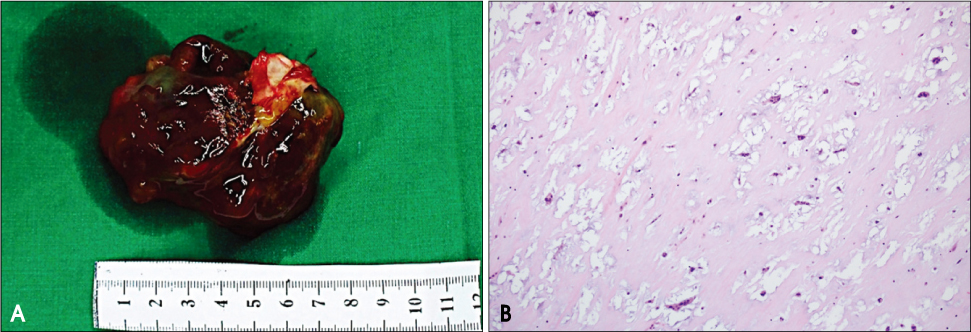
Fig. 4 The tumor had a polypoid shape and extensive hemorrhagic and myxoid appearance. (A, Gross findings. 7 × 4 × 3 cm in size, 76 grams). The tumor was composed of round, polygonal, stellate cells surrounded by abundant loose myxoid stroma. (B, Histologic findings. × 100, H & E stain).
Reference
-
1. Reynen K. Cardiac myxomas. N Engl J Med. 1995. 333:1610–1617.
Article2. Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma: a series of 112 consecutive cases. Medicine. 2001. 80:159–172.
Article3. Keeling IM, Oberwalder P, Anelli-Monti M, Schuchlenz H, Demel U, Tilz GP, Rehak P, Rigler B. Cardiac myxoma: 24 years of experience in 49 patients. Eur J Cardiothorac Surg. 2002. 22:971–977.4. M. Nadeem Attar, Roger K. Moore, Sarfraz Khan. Left atrial myxoma presenting with ventricular fibrillation. J Cardiovasc Med (Hagerstown). 2008. 9:282–284.
Article5. Marcus GM, Smith LM, Glidden DV, Wilson E, McCabe JM, Whiteman D, Tseng ZH, Badhwar N, Lee BK, Lee RJ, Scheinman MM, Olgin JE. Markers of inflammation before and after curative ablation of atrial flutter. Heart Rhythm. 2008. 5:215–221.
Article6. Mendoza CE, Rosado MF, Bemal L. The role of interleukin-6 in cases of cardiac myxoma: Clinical features, immunologic abnormalities, and a possible role in recurrence. Tex Heart Inst J. 2001. 28:3–7.7. Koo SH, Cha TJ, Choi YJ, Yoo CH, Kim HS, Heo JH, Nattel S, Lee JW. Evidence for a role of inflammation in atrial fibrillation associated with heart failure and the protective effects of angiotensin receptor blockade. Heart Rhythm. 2008. 5:S263.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Silent Left Large Atrial Myxoma: A Patient with Serial Electrocardiogram Variation
- Management of Atrial Flutter
- Recurred Right Atrial Myxoma after Resection of Left Atrial Myxoma (Recurred Myxoma): A case report
- A case of sinus node dysfunction and atrial tachycardia after the excision of a left atrial myxoma
- A case of fetal atrial flutter with hydrops fetalis
