Complete Fracture of Sirolimus-Eluting Stent in a Saphenous Vein Graft to Left Anterior Descending Artery
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. miinee@paran.com
- KMID: 1490701
- DOI: http://doi.org/10.4070/kcj.2009.39.6.251
Abstract
- Coronary stent fractures have been suggested as a potential new mechanism of restenosis. The mechanical properties of stents were designed not only to prevent vessel recoil, but also to resist the mechanical stress of vessel movement over millions of cardiac cycles. We present a case in which mechanical stress may have contributed to the fracture of a stent implanted in a saphenous vein graft (SVG) to the left coronary artery. The patient was admitted due to chest pain 2 years after receiving a coronary artery bypass graft. A coronary angiography revealed the culprit vessel to be the SVG to the left coronary artery. The graft was stenosed and was stented with a sirolimus-eluting stent. A 6-month follow-up coronary angiography revealed 80% in-stent restenosis with stent fracture. We re-intervened by balloon angioplasty. This is the first report of sirolimus-eluting stent fracture combined with restenosis of SVG in Korea.
MeSH Terms
Figure
-
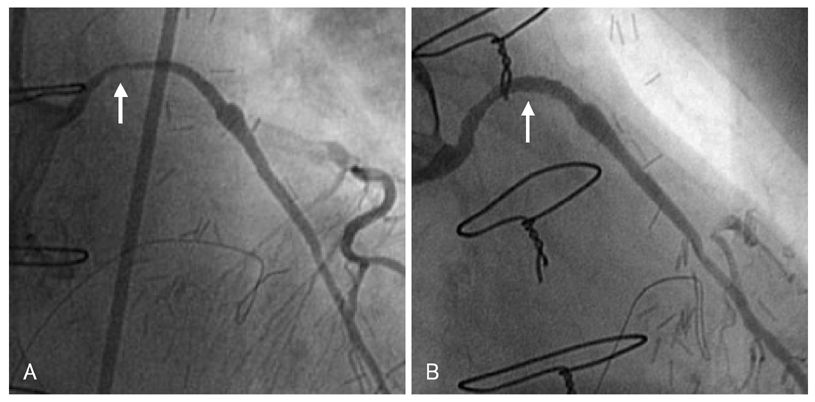
Fig. 1 Angiographic views of SVG to the left anterior descending artery during the initial coronary intervention. A: angiography revealed 70% focal stenosis of the proximal SVG to the left anterior descending artery (arrow). B: after SES implantation for the SVG, a well deployed stent without residual stenosis was evident (arrow). SVG: saphenous vein graft, SES: sirolimus-eluting stent.
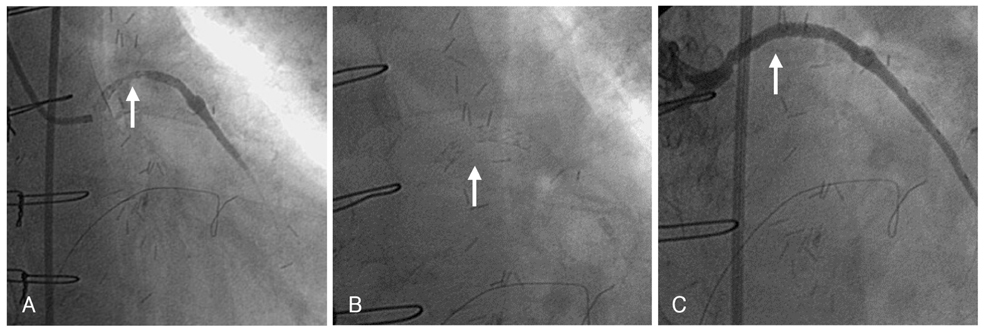
Fig. 2 Angiographic views of the SVG to the left anterior descending artery. A: angiography revealing 80% focal in-stent restenosis (arrow). B: complete strut fracture of mid portion of the Cypher stent was observed (arrow). C: final angiography after balloon angioplasty revealing good distal flow of the SVG without residual stenosis. SVG: saphenous vein graft.
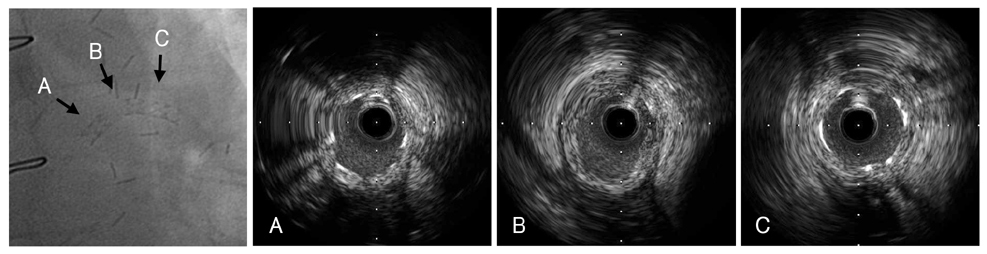
Fig. 3 Angiographic and intravascular ultrasound images on fractured stent at SVG. A: proximal stent segment. B: point of stent fracture (lack of stent layer). C: distal stent segment. SVG: saphenous vein graft.
Reference
-
1. Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003. 349:1315–1323.2. Kim JS, Yoon YW, Hong BK, et al. Delayed stent fracture after successful sirolimus-eluting stent (Cypher®) implantation. Korean Circ J. 2006. 36:443–449.3. Halkin A, Carlier S, Leon MB. Late incomplete lesion coverage following Cypher stent deployment for diffuse right coronary artery stenosis. Heart. 2004. 90:e45.4. Sianos G, Hofma S, Ligthart JM, et al. Stent fracture and restenosis in the drug-eluting stent era. Catheter Cardiovasc Interv. 2004. 61:111–116.5. Lee SY, Im E, Yang WI, Kim JS, Cho YH, Shim WH. A sirolimus-eluting stent fracture combined with a coronary artery aneurysm. Korean Circ J. 2008. 38:69–71.6. Ramana RK, Ronan A, Cohoon K, et al. Long-term clinical outcomes of real-world experience using sirolimus-eluting stents in saphenous vein graft disease. Catheter Cardiovasc Interv. 2008. 71:886–893.7. Vermeersch P, Agostoni P, Verheye S, et al. Increased late mortality after sirolimus-eluting stents versus bare-metal stents in diseased saphenous vein grafts: results from the randomized DELAYED PRISC trial. J Am Coll Cardiol. 2007. 50:261–267.8. Aoki J, Nakazawa G, Tanabe K, et al. Incidence and clinical impact of coronary stent fracture after sirolimus-eluting stent implantation. Catheter Cardiovasc Interv. 2007. 69:380–386.9. Yang TH, Kim DI, Park SG, et al. Clinical characteristics of stent fracture after sirolimus-eluting stent implantation. Int J Cardiol. 2009. 131:212–216.10. Okumura M, Ozaki Y, Ishii J, et al. Restenosis and stent fracture following sirolimus-eluting stent (SES) implantation. Circ J. 2007. 71:1669–1677.11. Lee MS, Jurewitz D, Aragon J, Forrester J, Makkar RR, Kar S. Stent fracture associated with drug-eluting stents: clinical characteristics and implications. Catheter Cardiovasc Interv. 2007. 69:387–394.12. Lemos PA, Saia F, Ligthart JM, et al. Coronary restenosis after sirolimus-eluting stent implantation: morphological description and mechanistic analysis from a consecutive series of cases. Circulation. 2003. 108:257–260.13. Koh TW, Mathur A. Coronary stent fracture in a saphenous vein graft to right coronary artery: successful treatment by the novel use of the Jomed coronary stent graft: case report and review of the literature. Int J Cardiol. 2007. 119:e43–e45.14. Duda SH, Pusich B, Richter G, et al. Sirolimus-eluting stents for the treatment of obstructive superficial femoral artery disease: six-month results. Circulation. 2002. 106:1505–1509.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of a Zotarolimus-Eluting Stent Fracture in the Left Anterior Descending Artery in a Patient Undergoing Hemodialysis
- Successful Management of a Rare Case of Stent Fracture and Subsequent Migration of the Fractured Stent Segment Into the Ascending Aorta in In-Stent Restenotic Lesions of a Saphenous Vein Graft
- Very Late Stent Thrombosis Related to Fracture of a Sirolimus-Eluting Stent
- A Case of Coronary Artery Aneurysm after Sirolimus-Eluting Stent Implantation
- Stent-Graft Repair of Common Carotid Pseudoaneurysms in Behcet's Syndrome
