Successful Management of a Rare Case of Stent Fracture and Subsequent Migration of the Fractured Stent Segment Into the Ascending Aorta in In-Stent Restenotic Lesions of a Saphenous Vein Graft
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea. mkhong61@yuhs.ac
- 2Severance Biomedical Science Institute, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2297910
- DOI: http://doi.org/10.4070/kcj.2012.42.1.58
Abstract
- Stent fracture is a complication following implantation of drug eluting stents and is recognized as one of the risk factors for in-stent restenosis. We present the first case of successfully managing a stent fracture and subsequent migration of the fractured stent into the ascending aorta that occurred during repeat revascularization for in-stent restenosis of an ostium of saphenous vein graft after implantation of a zotarolimus-eluting stent. Although the fractured stent segment had migrated into the ascending aorta with a pulled balloon catheter, it was successfully repositioned in the saphenous vein graft using an inflated balloon catheter. Then, the fractured stent segment was successfully connected to the residual segment of the zotarolimus-eluting stent by covering it with an additional sirolimuseluting stent.
MeSH Terms
Figure
-
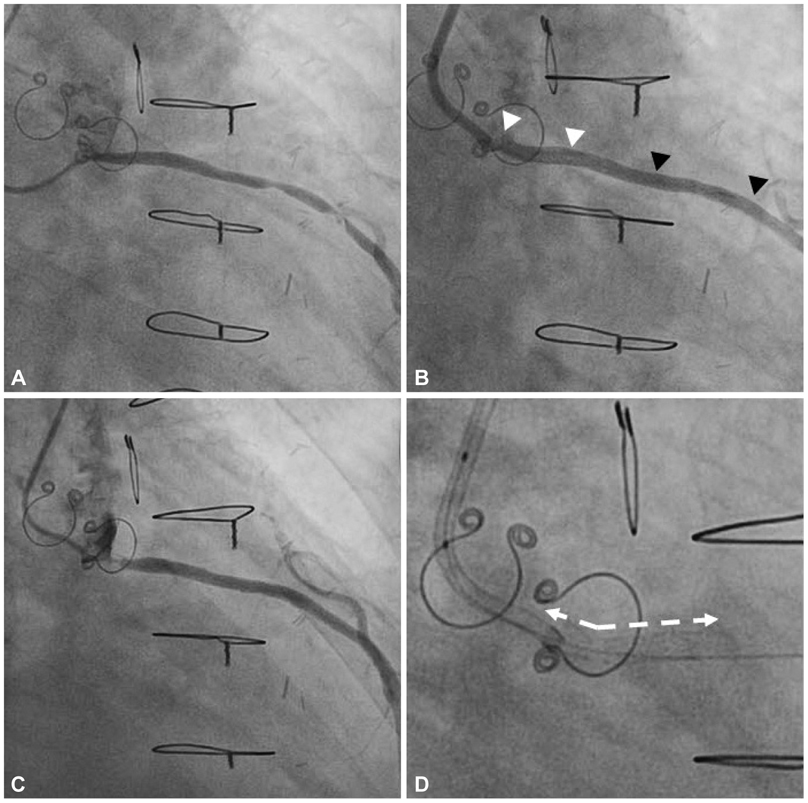
Fig. 1 Two significantly stenotic lesions were detected in the saphenous vein graft from the ascending aorta to the left anterior descending artery; 80% luminal narrowing at the ostium and 90% luminal narrowing at the mid-portion (A). These lesions were successfully treated with zotarolimus-eluting stent (ZES) (B). The 4-month follow-up angiogram after stent implantation showed 90% in-stent restenosis at the ostium and a patent stent at the mid-portion of the saphenous vein graft (C). Fluoroscopic images showed angulation (arrows with dotted line) of the proximal portion of the ZES at the ostium (D).
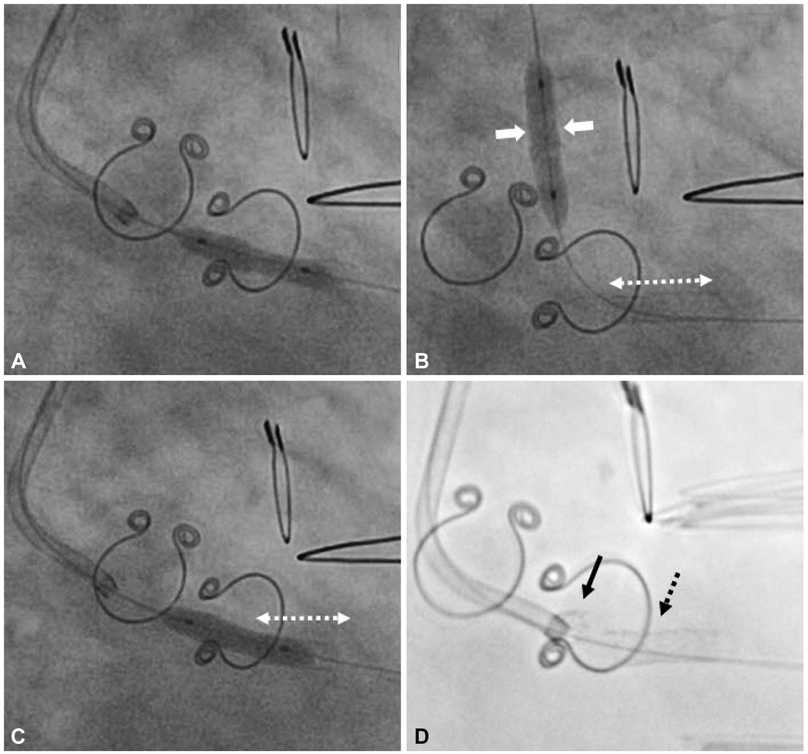
Fig. 2 Balloon angioplasty with a cutting balloon catheter was performed (A) A stent fracture occurred during adjunct balloon dilatation with a noncompliance balloon catheter and the fractured stent segment (two white thick arrows) had migrated into the ascending aorta along the inflated balloon catheter (B, arrow with dotted line: residual stent part). The migrated fractured struts were successfully pushed into the ostium of the saphenous vein graft without deflating the balloon catheter (C). Fluoroscopic image shows a gap between the fractured stent segment (black arrow with solid line) and the residual stent part (black arrow with dotted line) (D).
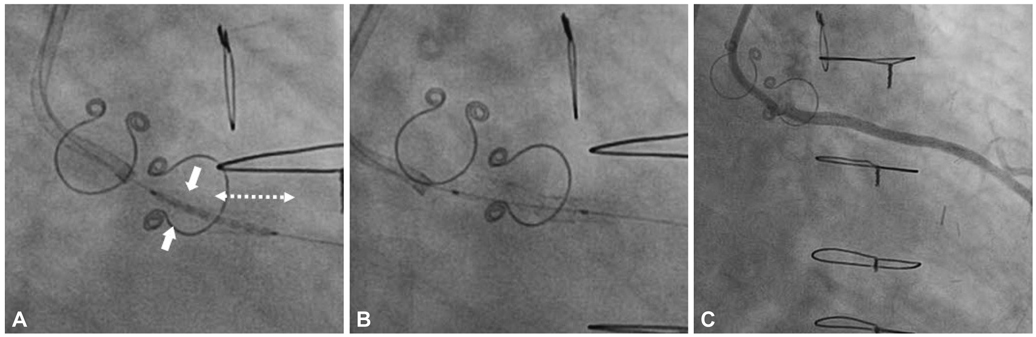
Fig. 3 A sirolimus-eluting stent was deployed connect the distal part of the fractured stent (two white thick arrows) with the proximal part of the residual stent (arrow with dotted line) to prevent systemic stent embolization (A). Fluoroscopic images after implantation of the sirolimus-eluting stent showed that the separated zotarolimus-eluting stent segments were well connected without a gap using an additional stent (B). Final angiogram revealed no residual stenosis (C).
Reference
-
1. Chakravarty T, White AJ, Buch M, et al. Meta-analysis of incidence, clinical characteristics and implications of stent fracture. Am J Cardiol. 2010. 106:1075–1080.2. Nakazawa G, Finn AV, Vorpahl M, et al. Incidence and predictors of drug-eluting stent fracture in human coronary artery a pathologic analysis. J Am Coll Cardiol. 2009. 54:1924–1931.3. Canan T, Lee MS. Drug-eluting stent fracture: incidence, contributing factors, and clinical implications. Catheter Cardiovasc Interv. 2010. 75:237–245.4. Sianos G, Hofma S, Ligthart JM, et al. Stent fracture and restenosis in the drug-eluting stent era. Catheter Cardiovasc Interv. 2004. 61:111–116.5. Aoki J, Nakazawa G, Tanabe K, et al. Incidence and clinical impact of coronary stent fracture after sirolimus-eluting stent implantation. Catheter Cardiovasc Interv. 2007. 69:380–386.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful coronary stent retrieval from the ascending aorta using a gooseneck snare kit
- Stent-Graft Repair of Common Carotid Pseudoaneurysms in Behcet's Syndrome
- Drug-Eluting Stent: Present and Future
- Treating a Ruptured Ascending Aorta with an Endovascular Stent Graft
- Jejunal Migration of the Stent-Graft Used for Common Hepatic Artery Pseudoaneurysm
