Role of Echocardiography in Patients with Acute Pulmonary Thromboembolism
- Affiliations
-
- 1Department of Internal Medicine, Chungnam National University, Daejeon, Korea. jaehpark@cnuh.co.kr
- KMID: 1486604
- DOI: http://doi.org/10.4250/jcu.2008.16.1.9
Abstract
- Acute pulmonary thromboembolism (PTE) is a common problem. In the emergency room, a substantial number of patients with chest discomfort have had an acute PTE. Presently, accepted diagnostic modalities for the confirmation of PTE include ventilation/perfusion (V/Q) scanning, chest computed tomography (CT), and standard angiography. However, each modality has important limitations. Although chest CT scanning has for the most part replaced lung scanning as the main diagnostic test for PTE, transthoracic echocardiography (TTE) is a noninvasive modality providing rapid results at the bedside. As well as being noninvasive modality, TTE avoids the contrast and radiation hazards of chest CT or conventional angiography. Thus echocardiography is an attractive imaging modality to diagnose PTE. TTE allows visualization of the aorta and the LV to evaluate for other etiologies of chest pain. Besides giving important diagnostic information, TTE can aid prediction of prognosis. Presence of RV dilatation and dysfunction is a poor prognostic sign and is the indicator for thrombolytic therapy. However, TTE has some limitations including poor imaging quality depending on the acoustic window and has a low sensitivity in detecting PTE.
MeSH Terms
Figure
-
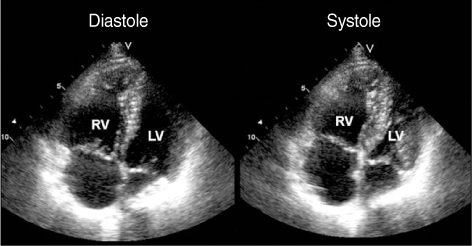
Fig. 1 Characteristic features of acute pulmonary thromboembolism identified by transthoracic echocardiography. Right ventricular dilatation and dysfunction were seen in a patient with acute pulmonary thromboembolism. In the diastole, the ratio of the right ventricular end-diastolic area to left ventricular end-diastolic area was more than 1.0 which is consistent with severe right ventricular dysfunction (normal value is less than 0.6).
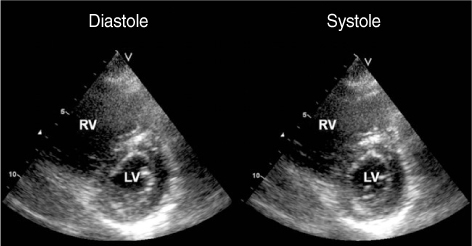
Fig. 2 Systolic and diastolic images with a parasternal short axis view from a patient with an acute pulmonary thromboembolism revealing septal flattening (D-shaped left ventricle) consistent with right ventricular pressure overload.
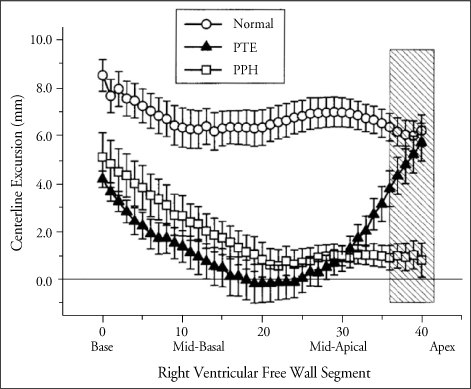
Fig. 3 McConnell's sign. Regional wall thickening fractions (mean±standard deviation) were presented in normal patients, patients with primary pulmonary hypertension (PPH), and those with a PTE. While apical wall motion was reduced in the PPH patients, it was intact in PTE patients. (Figure from McConnell MV, et al. Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism. Am J Cardiol 1996;78:469-73).

Fig. 4 Free-floating thrombi were found by transthoracic echocardiographic exam in a patient with acute pulmonary thromboembolism. A. A huge thrombus (arrows) was seen in the right atrium extended to right ventricle and crossing the tricuspid valve. B. After the opening of the right atrial wall, a worm like thrombus was found in the right atrium.
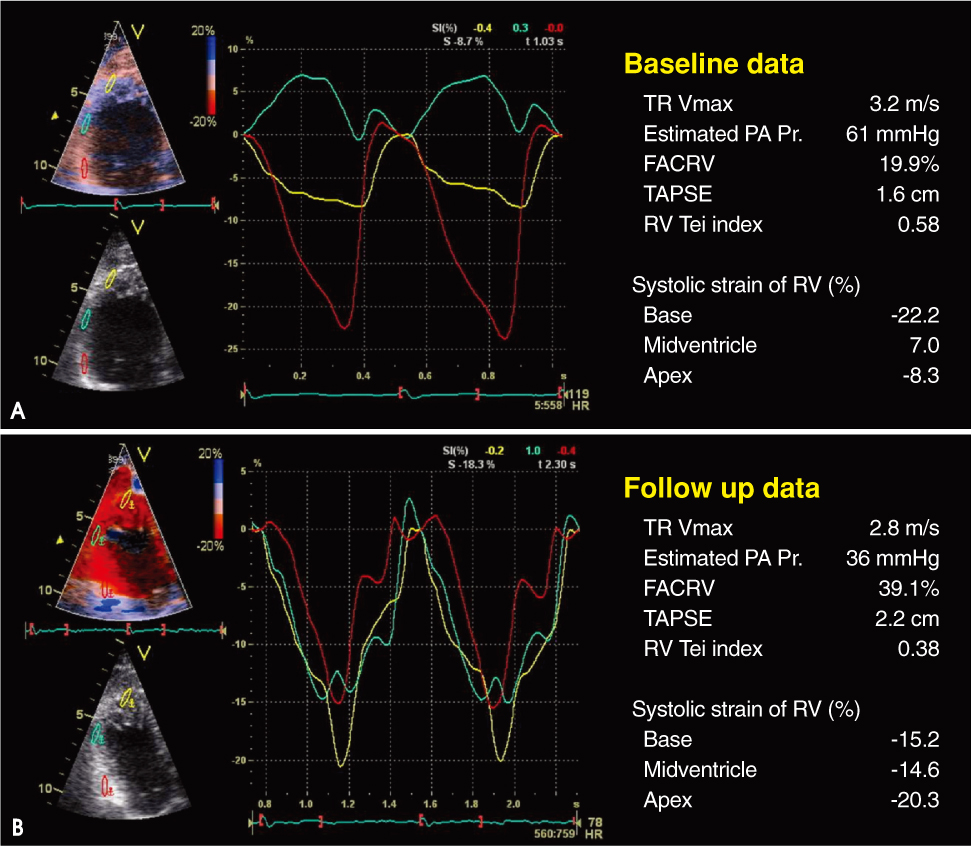
Fig. 5 Doppler tissue images of the right ventricular (RV) free wall were obtained using a low parasternal view, and three segments (apex, midventricle and base) were evaluated with an offset length of 12 mm. Baseline analysis showed decreased strain of the midventricle of the RV (A). Follow-up analysis showed increased strain of the midventricle with treatment (B). (Park JH, et al. Int J Cardiol 2008;125:319-24.)
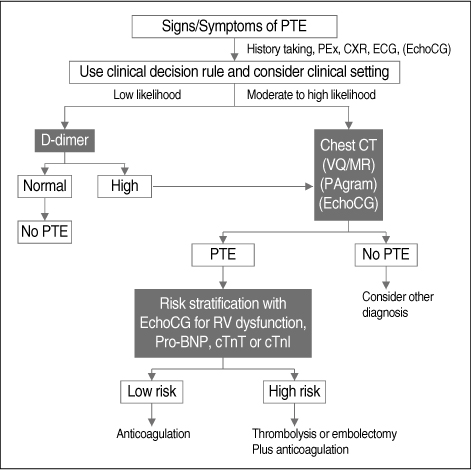
Fig. 6 A proposed algorithm of diagnosis and care for patient with an acute pulmonary thromboembolism (PTE). Imaging modality in the bracket is optional according to the clinical situation. PEx: physical examination, CXR: chest X-ray, ECG: electrocardiography, VQ: ventilation/perfusion scan, MR: magnetic resonance imaging, PAgram: pulmonary ateriogram, RV: right ventricle, pro-BNP: pro B type natriuretic peptide, cTnT: cardiac troponin T, cTnI: cardiac troponin I.
Cited by 2 articles
-
A Case of Consecutive Right and Left Ventricular Dysfunction
Seong-Mi Park, Jong-Il Choi, Soon-Jun Hong, Do-Sun Lim, Wan-Joo Shim
J Cardiovasc Ultrasound. 2008;16(4):123-125. doi: 10.4250/jcu.2008.16.4.123.Thrombus in Transit within a Patent Foramen Ovale: Gone with the Cough!
Ji-Hyun Kim, Yong-Jin Kim
J Cardiovasc Ultrasound. 2011;19(4):196-198. doi: 10.4250/jcu.2011.19.4.196.
Reference
-
1. Wood KE. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest. 2002. 121:877–905.2. Lilienfeld DE, Chan E, Ehland J, Godbold JH, Landrigan PJ, Marsh G. Mortality from pulmonary embolism in the United States: 1962 to 1984. Chest. 1990. 98:1067–1072.
Article3. Stein PD, Henry JW. Prevalence of acute pulmonary embolism among patients in a general hospital and at autopsy. Chest. 1995. 108:978–981.
Article4. Simonneau G, Azarian R, Brenot F, Dartevelle PG, Musset D, Duroux P. Surgical management of unresolved pulmonary embolism. A personal series of 72 patients. Chest. 1995. 107:52S–55S.5. Stein PD, Henry JW. Clinical characteristics of patients with acute pulmonary embolism stratified according to their presenting syndromes. Chest. 1997. 112:974–979.
Article6. Stein PD, Terrin ML, Hales CA, Palevsky HI, Saltzman HA, Thompson BT, Weg JG. Clinical, laboratory, roentgenographic, and electrocardiographic findings in patients with acute pulmonary embolism and no pre-existing cardiac or pulmonary disease. Chest. 1991. 100:598–603.
Article7. Konstantinides S. Pulmonary embolism: impact of right ventricular dysfunction. Curr Opin Cardiol. 2005. 20:496–501.
Article8. Rahimtoola A, Bergin JD. Acute pulmonary embolism: an update on diagnosis and management. Curr Probl Cardiol. 2005. 30:61–114.
Article9. Goldhaber SZ, Elliott CG. Acute pulmonary embolism: part I: epidemiology, pathophysiology, and diagnosis. Circulation. 2003. 108:2726–2729.10. Punukollu G, Gowda RM, Vasavada BC, Khan IA. Role of electrocardiography in identifying right ventricular dysfunction in acute pulmonary embolism. Am J Cardiol. 2005. 96:450–452.
Article11. The PIOPED Investigators. Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). JAMA. 1990. 263:2753–2759.12. Bone RC. Ventilation/perfusion scan in pulmonary embolism. 'The Emperor is incompletely attired'. JAMA. 1990. 263:2794–2795.
Article13. Kim KI, Muller NL, Mayo JR. Clinically suspected pulmonary embolism: utility of spiral CT. Radiology. 1999. 210:693–697.
Article14. Perrier A, Howarth N, Didier D, Loubeyre P, Unger PF, de Moerloose P, Slosman D, Junod A, Bounameaux H. Performance of helical computed tomography in unselected outpatients with suspected pulmonary embolism. Ann Intern Med. 2001. 135:88–97.
Article15. Anderson DR, Kahn SR, Rodger MA, Kovacs MJ, Morris T, Hirsch A, Lang E, Stiell I, Kovacs G, Dreyer J, Dennie C, Cartier Y, Barnes D, Burton E, Pleasance S, Skedgel C, O'Rouke K, Wells PS. Computed tomographic pulmonary angiography vs ventilation-perfusion lung scanning in patients with suspected pulmonary embolism: a randomized controlled trial. JAMA. 2007. 298:2743–2753.
Article16. Johnson TR, Nikolaou K, Wintersperger BJ, Knez A, Boekstegers P, Reiser MF, Becker CR. ECG-gated 64-MDCT angiography in the differential diagnosis of acute chest pain. AJR Am J Roentgenol. 2007. 188:76–82.
Article17. Dogan H, Kroft LJ, Huisman MV, van der Geest RJ, de Roos A. Right ventricular function in patients with acute pulmonary embolism: analysis with electrocardiography-synchronized multi-detector row CT. Radiology. 2007. 242:78–84.
Article18. Kluge A, Mueller C, Strunk J, Lange U, Bachmann G. Experience in 207 combined MRI examinations for acute pulmonary embolism and deep vein thrombosis. AJR Am J Roentgenol. 2006. 186:1686–1696.
Article19. Dalen JE, Brooks HL, Johnson LW, Meister SG, Szucs MM Jr, Dexter L. Pulmonary angiography in acute pulmonary embolism: indications, techniques, and results in 367 patients. Am Heart J. 1971. 81:175–185.
Article20. Kim EM, Park JH, Jang WI, Ahn KT, Kim MS, Kim KS, Jeong IS, Lee JH, Na KR, Seong IW. A case with acute pulmonary thromboembolism associated wtih nephrotic syndrome. J Cardiovasc Ultrasound. 2007. 15:101–104.
Article21. Goldhaber SZ. Thrombolysis for pulmonary embolism. N Engl J Med. 2002. 347:1131–1132.
Article22. Cheriex EC, Sreeram N, Eussen YF, Pieters FA, Wellens HJ. Cross sectional Doppler echocardiography as the initial technique for the diagnosis of acute pulmonary embolism. Br Heart J. 1994. 72:52–57.
Article23. Come PC. Echocardiographic evaluation of pulmonary embolism and its response to therapeutic interventions. Chest. 1992. 101:151S–162S.
Article24. Jardin F, Dubourg O, Gueret P, Delorme G, Bourdarias JP. Quantitative two-dimensional echocardiography in massive pulmonary embolism: emphasis on ventricular interdependence and leftward septal displacement. J Am Coll Cardiol. 1987. 10:1201–1206.
Article25. Kasper W, Geibel A, Tiede N, Bassenge D, Kauder E, Konstantinides S, Meinertz T, Just H. Distinguishing between acute and subacute massive pulmonary embolism by conventional and Doppler echocardiography. Br Heart J. 1993. 70:352–356.
Article26. Kreit JW. The impact of right ventricular dysfunction on the prognosis and therapy of normotensive patients with pulmonary embolism. Chest. 2004. 125:1539–1545.
Article27. McConnell MV, Solomon SD, Rayan ME, Come PC, Goldhaber SZ, Lee RT. Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism. Am J Cardiol. 1996. 78:469–473.
Article28. Miniati M, Monti S, Pratali L, Di Ricco G, Marini C, Formichi B, Prediletto R, Michelassi C, Di Lorenzo M, Tonelli L, Pistolesi M. Value of transthoracic echocardiography in the diagnosis of pulmonary embolism: results of a prospective study in unselected patients. Am J Med. 2001. 110:528–535.
Article29. Kircher BJ, Himelman RB, Schiller NB. Noninvasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am J Cardiol. 1990. 66:493–496.
Article30. Chan KL, Currie PJ, Seward JB, Hagler DJ, Mair DD, Tajik AJ. Comparison of three Doppler ultrasound methods in the prediction of pulmonary artery pressure. J Am Coll Cardiol. 1987. 9:549–554.
Article31. Masuyama T, Kodama K, Kitabatake A, Sato H, Nanto S, Inoue M. Continuous-wave Doppler echocardiographic detection of pulmonary regurgitation and its application to noninvasive estimation of pulmonary artery pressure. Circulation. 1986. 74:484–492.
Article32. Lee JH, Park JH, Kim EM, Jang WI, Ahn KT, Kim MS, Kim KS, Jeong IS, Jeong JO, Seong IW. Prelude of tragedy: Entrapped huge thrombi into a patent foramen ovale impending paradoxical embolism. J Cardiovasc Ultrasound. 2007. 15:121–123.
Article33. lee KH, Hwang SO, Kim YS, Ahn ME, Cho YK, Yoon JH, Park KS, Choe KH. Thrombi in main pulmonary artery detected by echocardiography. J Kor Soc Echo. 1994. 2:225–228.
Article34. Lee BH, Son IS, Kim SJ, Moon JY, Kang HS, Choue CW, Kim KS, Song JS, Bae JH. A case of pulmonary artery sarcoma with cancer pulmonary embolism. J Kor Soc Echo. 2003. 11:124–127.35. Grifoni S, Olivotto I, Cecchini P, Pieralli F, Camaiti A, Santoro G, Pieri A, Toccafondi S, Magazzini S, Berni G, Agnelli G. Utility of an integrated clinical, echocardiographic, and venous ultrasonographic approach for triage of patients with suspected pulmonary embolism. Am J Cardiol. 1998. 82:1230–1235.
Article36. Jackson RE, Rudoni RR, Hauser AM, Pascual RG, Hussey ME. Prospective evaluation of two-dimensional transthoracic echocardiography in emergency department patients with suspected pulmonary embolism. Acad Emerg Med. 2000. 7:994–998.
Article37. Stawicki SP, Seamon MJ, Kim PK, Meredith DM, Chovanes J, Schwab CW, Gracias VH. Transthoracic echocardiography for pulmonary embolism in the ICU: finding the "right" findings. J Am Coll Surg. 2008. 206:42–47.
Article38. Arcasoy SM, Vachani A. Local and systemic thrombolytic therapy for acute venous thromboembolism. Clin Chest Med. 2003. 24:73–91.
Article39. Yip G, Abraham T, Belohlavek M, Khandheria BK. Clinical applications of strain rate imaging. J Am Soc Echocardiogr. 2003. 16:1334–1342.
Article40. Sutherland GR, Di Salvo G, Claus P, D'Hooge J, Bijnens B. Strain and strain rate imaging: a new clinical approach to quantifying regional myocardial function. J Am Soc Echocardiogr. 2004. 17:788–802.
Article41. Kjaergaard J, Sogaard P, Hassager C. Right ventricular strain in pulmonary embolism by Doppler tissue echocardiography. J Am Soc Echocardiogr. 2004. 17:1210–1212.
Article42. Park JH, Park YS, Park SJ, Lee JH, Choi SW, Jeong JO, Seong IW. Midventricular peak systolic strain and Tei index of the right ventricle correlated with decreased right ventricular systolic function in patients with acute pulmonary thromboembolism. Int J Cardiol. 2008. 125:319–324.
Article43. Hsiao SH, Chang SM, Lee CY, Yang SH, Lin SK, Chiou KR. Usefulness of tissue Doppler parameters for identifying pulmonary embolism in patients with signs of pulmonary hypertension. Am J Cardiol. 2006. 98:685–690.
Article44. Leibowitz D. Role of echocardiography in the diagnosis and treatment of acute pulmonary thromboembolism. J Am Soc Echocardiogr. 2001. 14:921–926.
Article45. Rosenberger P, Shernan SK, Body SC, Eltzschig HK. Utility of intraoperative transesophageal echocardiography for diagnosis of pulmonary embolism. Anesth Analg. 2004. 99:12–16.
Article46. Dalen JE, Alpert JS, Hirsh J. Thrombolytic therapy for pulmonary embolism: is it effective? Is it safe? When is it indicated? Arch Intern Med. 1997. 157:2550–2556.
Article47. Toosi MS, Merlino JD, Leeper KV. Prognostic value of the shock index along with transthoracic echocardiography in risk stratification of patients with acute pulmonary embolism. Am J Cardiol. 2008. 101:700–705.
Article48. Grifoni S, Olivotto I, Cecchini P, Pieralli F, Camaiti A, Santoro G, Conti A, Agnelli G, Berni G. Short-term clinical outcome of patients with acute pulmonary embolism, normal blood pressure, and echocardiographic right ventricular dysfunction. Circulation. 2000. 101:2817–2822.
Article49. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999. 353:1386–1389.
Article50. Binder L, Pieske B, Olschewski M, Geibel A, Klostermann B, Reiner C, Konstantinides S. N-terminal pro-brain natriuretic peptide or troponin testing followed by echocardiography for risk stratification of acute pulmonary embolism. Circulation. 2005. 112:1573–1579.
Article51. Scridon T, Scridon C, Skali H, Alvarez A, Goldhaber SZ, Solomon SD. Prognostic significance of troponin elevation and right ventricular enlargement in acute pulmonary embolism. Am J Cardiol. 2005. 96:303–305.
Article52. Goldhaber SZ. Echocardiography in the management of pulmonary embolism. Ann Intern Med. 2002. 136:691–700.
Article53. Johnson ME, Furlong R, Schrank K. Diagnostic use of emergency department echocardiogram in massive pulmonary emboli. Ann Emerg Med. 1992. 21:760–763.
Article54. Pruszczyk P, Torbicki A, Kuch-Wocial A, Chlebus M, Miskiewicz ZC, Jedrusik P. Transoesophageal echocardiography for definitive diagnosis of haemodynamically significant pulmonary embolism. Eur Heart J. 1995. 16:534–538.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Multiple Myeloma with Pulmonary Thromboembolism Diagnosed by Transthoracic Echocardiography
- Thrombi in Main Pulmonary Artery Detected by Echocardiography
- Acute Massive Pulmonary Thromboembolism Occurring during Femur Surgery: The Key Role of Transesophageal Echocardiography : A case report
- The Prognostic Role of B-type Natriuretic Peptide in Acute Pulmonary Thromboembolism
- Pulmonary Thromboembolism and Infarction Caused by Right-Sided Infective Endocarditis in a Patient with Ventricular Septal Defect
