Variations in Sagittal Spinopelvic Parameters According to the Lumbar Spinal Morphology in Healthy Korean Young Men
- Affiliations
-
- 1Department of Orthopaedic Surgery, National Police Hospital, Seoul, Korea.
- 2Department of Orthopaedic Surgery, Seoul Veterans Hospital, Seoul, Korea. drortho@korea.com
- 3Department of Orthopaedic Surgery, Columbia University Medical Center, NY, USA.
- KMID: 1459270
- DOI: http://doi.org/10.4184/jkss.2010.17.2.66
Abstract
- STUDY DESIGN: This is a prospective radiographic study.
OBJECTIVES
We wanted to describe and quantify the common variations in the sagittal lumbar spine. SUMMARY OF THE LITERATURE REVIEW: No previous study of the spinopelvic parameters with a large cohort of asymptomatic young men was performed on subjects with the same ethnic background.
MATERIALS AND METHODS
166 young males without disease, trauma or a history of operation on the spine or lower extremities were included. The sagittal standing radiographs of the whole spine on 36 inch film were taken. The distances from the plumb line of C7, T12, the lumbar apex and the bicoxofemoral head to the posterosuperior corner of the sacrum were measured. Thoracic kyphosis, thoracolumbar kyphosis, lumbar lordosis, the segmental vertebral slopes, the sacral slope and the pelvic incidence were measured. Groups 1 and 2 were classified by having a sacral slope less than 35degrees (group 1: apex below L4, group 2: above L4). Group 3 had a sacral slope between 35degrees and 45degrees, and group 4 had a sacral slope greater than 45degrees.
RESULTS
The average age was 21.8 years (range: 19~26 years). Group 1 contained 37 cases, group 2 had 44, group 3 had 62 and group 4 had 23. Thoracolumbar kyphosis was significantly increased in group 1 and lumbar lordosis and pelvic incidence were increased in groups 3 and 4. Thoracic kyphosis and the vertebral slope of T12 did not demonstrate any difference between the groups.
CONCLUSION
The sagittal spinopelvic parameters showed significant changes according to the morphology of the lower lumbar spine. Understanding the patterns of variation in the spinopelvic parameters may help surgeons to plan treatment for various spinal lesions.
Keyword
MeSH Terms
Figure
-
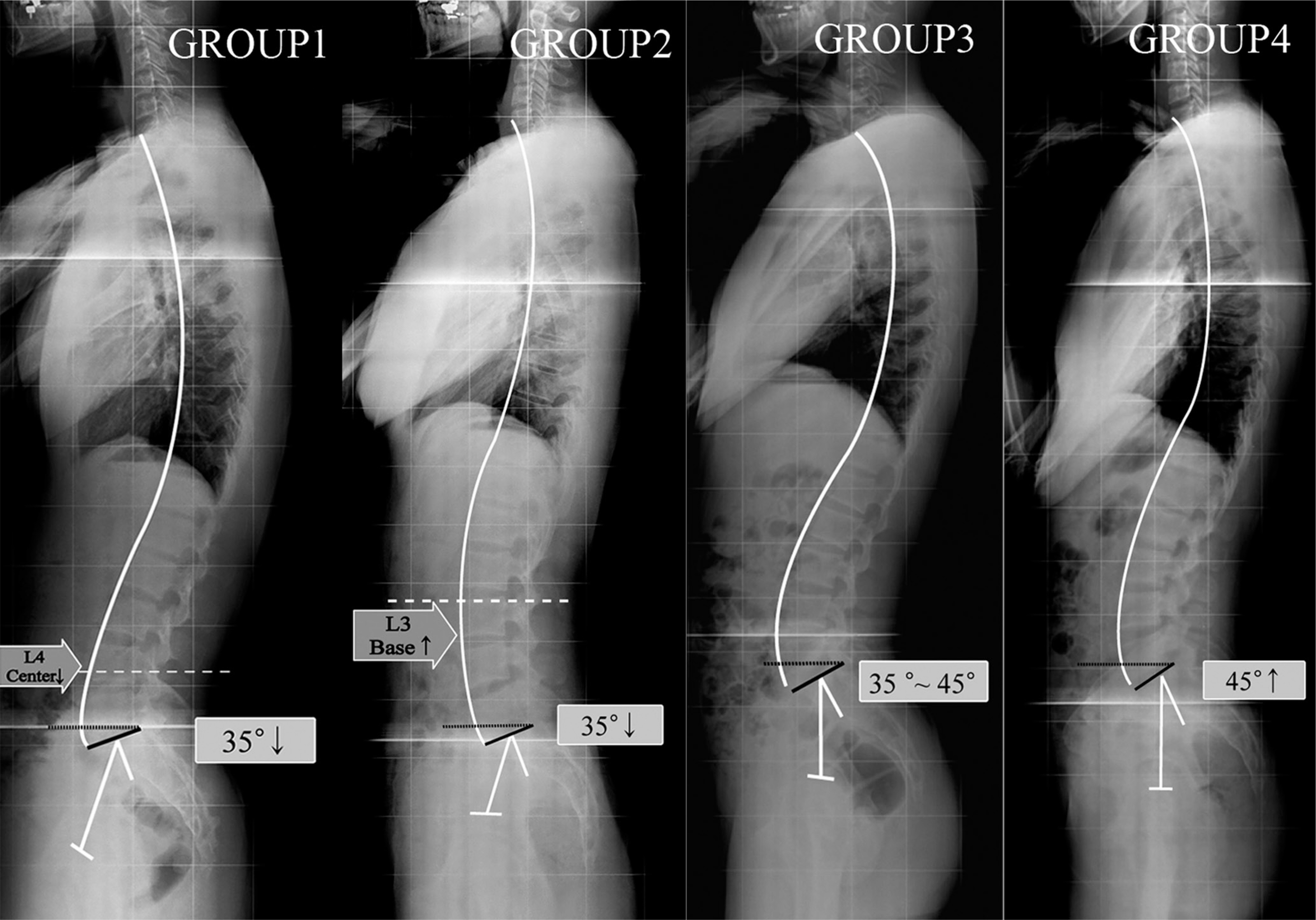
Fig.1. A four-part classification of the normal variation in the sagittal spinopelvic alignment in the standing position. Group 1. Sacral slope is less than 35° and the apex of lumbar lordosis is below L4 center. Group 2. Sacral slope is less than 35° and the apex of lumbar lordosis is above L4 base. Group 3 includes subjects with sacral slope from 35° to 45°, and Group 4 with sacral slope above 45°.

Fig.2. The method of measuring the sagittal parameters. (A) The distances from the plumbs of C7 (a), T12 (b), Lumbar apex (c) and bicoxofemoral (d) to the posterosuperior corner of sacrum are measured. A positive value means forward transition and a negative value means backward transition. (B) The vertebral slopes are measured in T5 upper end plate (UEP), T10 UEP, T12 lower end plate (LEP), L2 LEP, L4 UEP. A positive value means vertebral slope is below the horizontal line. (C) The angular parameters are given by vertebral slopes. Thoracic kyphosis (TK, T5 UEP - T12 LEP), thoracolumbar kyphosis (TLK, T10 UEP - L2 LEP), total lumbar lordosis (LL, T12 LEP – S1 UEP) are measured. (D) Sacral slope (SS) and pelvic incidence (PI) are measured for the pelvic parameters.
Cited by 2 articles
-
A Comparative Analysis of Thoracic and Thoracolumbar Kyphosis between Young Men and Old Men
Gyu-Bok Kang, Young-Joon Ahn, Yongjung J. Kim, Youngbae B. Kim, Young-Rok Ko
J Korean Orthop Assoc. 2016;51(1):48-53. doi: 10.4055/jkoa.2016.51.1.48.Changes in Sagittal Spinopelvic Parameters according to Pelvic Incidence in Asymptomatic Old Korean Men
Kyu-Bok Kang, Young-Jun Ahn, Yongjung J Kim, Young-Bae Kim, Sung-Chul Park
J Korean Soc Spine Surg. 2011;18(4):223-229. doi: 10.4184/jkss.2011.18.4.223.
Reference
-
1.Stagnara P., De Mauroy JC., Dran G, et al. Reciprocal angulation of vertebral bodies in a sagittal plane: approach to references for the evaluation of kyphosis and lordosis. Spine. 1982. 7:335–42.
Article2.Bernhardt M., Bridwell KH. Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine. 1989. 14:717–21.
Article3.Jackson RP., McManus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine. 1994. 19:1611–8.4.Gelb DE., Lenke LG., Bridwell KH., Blanke K., McEnery KW. An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine. 1995. 20:1351–8.
Article5.Korovessis PG., Stamatakis MV., Baikousis AG. Reciprocal angulation of vertebral bodies in the sagittal plane in an asymptomatic Greek population. Spine. 1998. 23:700–4.
Article6.Roussouly P., Gollogly S., Berthonnaud E., Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine. 2005. 30:346–53.
Article7.Boulay C., Tardieu C., Hecquet J, et al. Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis. Eur Spine J. 2006. 15:415–22.
Article8.Smith A., O'Sullivan P., Straker L. Classification of sagittal thoraco-lumbo-pelvic alignment of the adolescent spine in standing and its relationship to low back pain. Spine. 2008. 33:2101–7.
Article9.O'Brien MF., Kuklo TR., Blanke KM., Lenke LG. Radiographic Measurement Manual. Spinal Deformity Study Group(SDSG). Medtronic Sofamor Danek. 2004.10.Troyanovich SJ., Cailliet R., Janik TJ., Harrison DD., Harrison DE. Radiographic mensuration characteristics of the sagittal lumbar spine from a normal population with a method to synthesize prior studies of lordosis. J Spinal Disord. 1997. 10:380–6.
Article11.Vedantam R., Lenke LG., Keeney JA., Bridwell KH. Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine. 1998. 23:211–5.
Article12.Jackson RP., Kanemura T., Kawakami N., Hales C. Lumbopelvic lordosis and pelvic balance on repeated standing lateral radiographs of adult volunteers and untreated patients with constant low back pain. Spine. 2000. 25:575–86.
Article13.Hammerberg EM., Wood KB. Sagittal profile of the elderly. J Spinal Disord Tech. 2003. 16:44–50.
Article14.Kobayashi T., Atsuta Y., Matsuno T., Takeda N. A longitudinal study of congruent sagittal spinal alignment in an adult cohort. Spine. 2004. 29:671–6.
Article15.Mac-Thiong JM., Berthonnaud E., Dimar JR., Betz RR., Labelle H. Sagittal alignment of the spine and pelvis during growth. Spine. 2004. 29:1642–7.
Article16.Vialle R., Levassor N., Rillardon L., Templier A., Skalli W., Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am. 2005. 87:260–7.
Article17.Lee CS., Oh WH., Chung SS., Lee SG., Lee JY. Analysis of the Sagittal Alignment of Normal Spines. J Korean Orthop Assoc. 1999. 34:949–54.
Article18.Kim WJ., Kang JW., Yeom JS, et al. A comparative analysis of sagittal spinal balance in 100 asymptomatic young and older aged volunteers. J Korean Soc Spine Surg. 2003. 10:327–34.
Article19.Jackson RP., Peterson MD., McManus AC., Hales C. Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordosis to the pelvic radius on standing lateral radiographs of adult volunteers and patients. Spine. 1998. 23:1750–67.
Article20.Vaz G., Roussouly P., Berthonnaud E., Dimnet J. Sagittal morphology and equilibrium of pelvis and spine. Eur Spine J. 2002. 11:80–7.
Article21.Berthonnaud E., Dimnet J., Roussouly P., Labelle H. Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disord Tech. 2005. 18:40–7.
Article22.Horton WC., Brown CW., Bridwell KH., Glassman SD., Suk SI., Cha CW. Is there an optimal patient stance for obtaining a lateral 36” radiograph? A critical comparison of three techniques. Spine. 2005. 30:427–33.23.Kim MS., Chung SW., Hwang CJ., Lee CK., Chang BS. A radiographic analysis of sagittal spinal alignment for the standardization of standing lateral position. J Korean Orthop Assoc. 2005. 40:861–8.
Article24.Kim YJ., Bridwell KH., Lenke LG., Kim YB., Ahn YJ. Comparative radiographic analysis of the sagittal spinopelvic alignment between 100 asymptomatic adults and 100 patients with sagittal imbalance. Poster session presented at: 2008 annual meeting. International Meeting on Advanced Spine Technology (IMAST);. 2008 July 8-11. Hong Kong. [E-Poster presentation E-Poster #419].25.Berlemann U., Jeszenszky DJ., Buhler DW., Harms J. The role of lumbar lordosis, vertebral end-plate inclination, disc height, and facet orientation in degenerative spondylolisthesis. J Spinal Disord. 1999. 12:68–73.
Article26.Legaye J., Duval-Beaupere G., Hecquet J., Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998. 7:99–103.
Article27.Lee CS., Chung SS., Chung KH., Kim SR. Significance of Pelvic Incidence in the Development of Abnormal Sagittal Alignment. J Korean Orthop Assoc. 2006. 41:274–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Sagittal Spinopelvic Alignment between Lumbar Degenerative Spondylolisthesis and Degenerative Spinal Stenosis
- The Comparison of Sagittal Spinopelvic Parameters between Young Adult Patients with L5 Spondylolysis and Age-Matched Control Group
- Correlates of Bone Mineral Density and Sagittal Spinal Balance in the Aged
- Changes of Spinopelvic Parameter using Iliac Screw In Surgical Correction of Sagittal Imbalance Patients
- Sagittal Balance, Pulmonary Function, and Spinopelvic Parameters in Severe Post-Tubercular Thoracic Kyphosis
