Cystic Pulmonary Metastasis in a Patient with Scalp Angiosarcoma: A Case Report
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kyungs.lee@samsung.com
- 2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 5Department of Otorhinolaryngology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1443477
- DOI: http://doi.org/10.3348/jksr.2011.65.2.143
Abstract
- It has been well known that angiosarcoma (AS), particularly scalp AS, metastasizes to the lungs with multiple air-filled cystic lesions on chest computed tomography scans. Pneumothorax, due to cystic lesion rupture into the pleural space, is frequent; however, we do not exactly know how rapidly the metastatic lesions spread to the lungs or what the exact pathogenetic mechanism for cystic metastasis is. According to our experience, the speed of disease progression in pulmonary metastasis is relatively fast and the entire lungs may be involved within two or three months. The infiltrating spindle cell tumors in the alveolar walls are tethering the adjacent alveolar spaces in order to form a dilated air-filled cystic lesion.
MeSH Terms
Figure
-
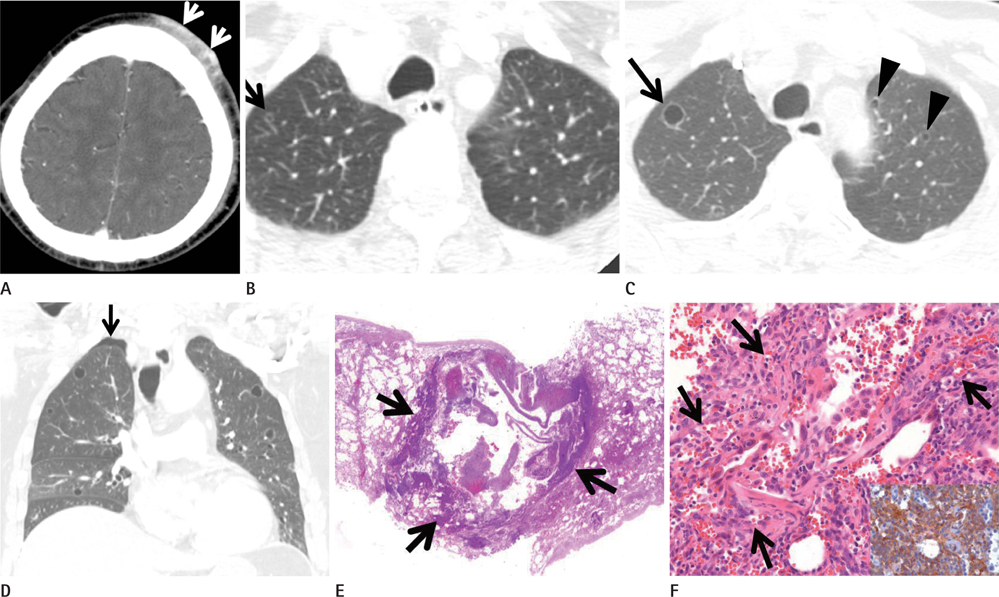
Fig. 1 Scalp angiosarcoma and cystic pulmonary metastasis in an 82-year-old man. A. Enhanced brain CT (5-mm-section thickness) shows an enhancing scalp lesion (arrows) in the left forehead area. B. Lung window image of thoracic CT (5.0-mm-section thickness) obtained at the same time to A demonstrates a 4-mm-sized air-filled cystic le-sion (arrow) in the right upper lobe. C. Follow-up chest CT images (2.5-mm-section thickness) obtained at the same level to B, and two months after A and B, demonstrate the enlargement of a cystic lesion (arrow) in the right upper lobe along with additional multiple cystic lesions (arrowheads) in both lungs. D. Coronal reformatted image (2.0-mm-section thickness) shows multiple cystic lesions in both lungs along with right pneumothorax (arrow). E, F. Histopathologic and immunohistochemical staining for a surgical lung biopsy specimen. E. Scanning view (H & E, × 1) of histopathologic specimen discloses a cystic lesion, the wall of which is composed of alveolar wall structures (ar-rows) containing infiltrating spindle cell tumors. The cyst has internal hemorrhage. F. High-magnification view (H & E, × 200) reveals alveolar walls containing spindle-shaped or oval tumor cells forming slit-like vascular structures (arrows). The proliferated vasculature contains intraluminal red blood cells. Inset. strongly positive for CD31 on immunohistochemical staining.
Reference
-
1. Mark RJ, Tran LM, Sercarz J, Fu YS, Calcaterra TC, Juillard GF. Angiosarcoma of the head and neck. The UCLA experience 1955 through 1990. Arch Otolaryngol Head Neck Surg. 1993; 119:973–997.2. Morgan MB, Swann M, Somach S, Eng W, Smoller B. Cutaneous angiosarcoma: a case series with prognostic correlation. J Am Acad Dermatol. 2004; 50:867–874.3. Kitagawa M, Tanaka I, Takemura T, Matsubara O, Kasuga T. Angiosarcoma of the scalp: report of two cases with fatal pulmonary complications and a review of Japanese autopsy registry data. Virchows Arch A Pathol Anat Histopathol. 1987; 412:83–87.4. Tateishi U, Hasegawa T, Kusumoto M, Yamazaki N, Iinuma G, Muramatsu Y, et al. Metastatic angiosarcoma of the lung: spectrum of CT findings. AJR Am J Roentgenol. 2003; 180:1671–1674.5. Kim MY, Lim BS, Oh MH, Im JG. Metastatic angiosarcoma of the lung: HRCT findings. J Korean Radiol Soc. 1999; 40:493–496.6. Park SI, Choi E, Lee HB, Rhee YK, Chung MJ, Lee YC. Spontaneous pneumomediastinum and hemopneumothoraces secondary to cystic lung metastasis. Respiration. 2003; 70:211–213.7. Lawton PA, Knowles S, Karp SJ, Suvana SK, Spittle MF. Bilateral pneumothorax as a presenting feature of metastatic angiosarcoma of the scalp. Br J Radiol. 1990; 63:132–134.8. Lee CH, Park KU, Nah DY, Won KS. Bilateral spontaneous pneumothorax during cytotoxic chemotherapy for angiosarcoma of the scalp: a case report. J Korean Med Sci. 2003; 18:277–280.9. Goto H, Watanuki Y, Miyazawa N, Kudo M, Inoue S, Kobayashi N, et al. [Clinical and pathological analysis of 10 cases of secondary pneumothorax due to angiosarcoma of the scalp]. Nihon Kokyuki Gakkai Zasshi. 2008; 46:85–91.10. Lahat G, Dhuka AR, Lahat S, Smith KD, Pollock RE, Hunt KK, et al. Outcome of locally recurrent and metastatic angiosarcoma. Ann Surg Oncol. 2009; 16:2502–2509.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Emphysematous Cystic Pulmonary Metastasis of Angiosarcoma
- Pulmonary Metastasis in Angiosarcoma of the Scalp
- A Case of Pneumothorax Caused by Cystic Lung Metastasis of Angiosarcoma
- Cutaneous Angiosarcoma of the Scalp Aggravated after Hair Dyeing Presenting as Bilateral Facial Cellulitis: A Case Report
- Cutaneous Metastasis of Lung Angiosarcoma to the Scalp
