Decompressive Hemicraniectomy and Duroplasty in Toddlers and Preschool Children with Refractory Intracranial Hypertension after Unilateral Hemispheric Stroke
- Affiliations
-
- 1Department of Neurosurgery, Korea University Ansan Hospital, Ansan, Korea. neuron19@korea.ac.kr
- KMID: 1441415
- DOI: http://doi.org/10.3340/jkns.2012.51.2.86
Abstract
OBJECTIVE
Life-threatening hemispheric stroke is associated with a high mortality and morbidity. Decompressive hemicraniectomy has been regarded as an effective treatment option for refractory intracranial hypertension. Here, we reported the clinical course of 5 children with decompressive craniectomy and duroplasty after non-traumatic refractory intracranial hypertension.
METHODS
Four toddlers and one preschool-girl were included in this study; there were 3 boys and 2 girls with a mean age of 34.6 months (range 17-80). Decompressive craniectomy including duroplasty was performed in cases of dilatation of pupil size after intensified standard medical therapy had proven insufficient. All children had a Pediatric Glasgow Coma Scale score <8 at pre-operation state. The mean time-point of craniectomy after stroke attack was 12 hours (range 4-19).
RESULTS
During the long-term follow-up period (mean 47.6 months), no children died. One year later, when we checked their Glasgow Outcome Scale scores, only one toddler received a score of 4 (moderate disability). But the others had good recoveries although they had minor physical or mental deficits. According to the Pediatric Cerebral Performance Category Scale, 4 children received a score of 2 (mild disability).
CONCLUSION
Despite our small cases, we suggest that decompressive hemicraniectomy and duroplasty is an acceptable and life-saving treatment for refractory intracranial hypertension after unilateral hemispheric stroke in toddlers and preschool children.
Keyword
MeSH Terms
Figure
-
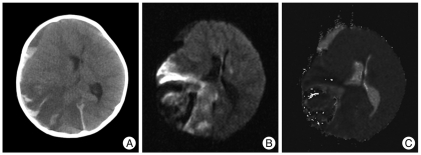
Fig. 1 A : Non enhanced brain CT revealed an acute right-sided middle cerebral artery territory infarct with mass effect manifested as right lateral ventricular compression, attenuation of the basal cisterns and right convexity sulci effacement. Because of midline shift due to severe brain parenchymal swelling, posterior horn of lateral ventricle was not seen. And hemorrhagic transformation was also noted at same side area. B and C : DWI MRI scan of his brain revealed that lesion was appropriate for acute cerebral infarction with hemorrhagic transformation with significant mid-line shift. CT : computed tomography, DWI : diffusion weighted image, MRI : magnetic resonance imaging.

Fig. 2 Brain CT at the time of post-operative 7 days revealed sustained brain swelling with decompressive craniectomy, but midline shift did not noted anymore.

Fig. 3 Three years later, there was encephalomalasic change in right-sided middle cerebral artery territory. The bone flap was secured.
Reference
-
1. Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the early management of adults with ischemic stroke : a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups : The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007; 115:e478–e534. PMID: 17515473.2. Aghakhani N, Durand P, Chevret L, Parker F, Devictor D, Tardieu M, et al. Decompressive craniectomy in children with nontraumatic refractory high intracranial pressure. Clinical article. J Neurosurg Pediatr. 2009; 3:66–69. PMID: 19119908.
Article3. Carter BS, Ogilvy CS, Candia GJ, Rosas HD, Buonanno F. One-year outcome after decompressive surgery for massive nondominant hemispheric infarction. Neurosurgery. 1997; 40:1168–1175. discussion 1175-1176. PMID: 9179889.
Article4. Chesnut RM. The management of severe traumatic brain injury. Emerg Med Clin North Am. 1997; 15:581–604. PMID: 9255134.
Article5. Chi CS, Law KL, Wong TT, Su GY, Lin N. Continuous monitoring of intracranial pressure in Reye's syndrome--5 years experience. Acta Paediatr Jpn. 1990; 32:426–434. PMID: 2288226.
Article6. Cho DY, Chen TC, Lee HC. Ultra-early decompressive craniectomy for malignant middle cerebral artery infarction. Surg Neurol. 2003; 60:227–232. discussion 232-233. PMID: 12922040.
Article7. Gordon AL, Ganesan V, Towell A, Kirkham FJ. Functional outcome following stroke in children. J Child Neurol. 2002; 17:429–434. PMID: 12174963.
Article8. Greenwood J Jr. Acute brain infarctions with high intracranial pressure : surgical indications. Johns Hopkins Med J. 1968; 122:254–260. PMID: 5655168.9. Gupta R, Connolly ES, Mayer S, Elkind MS. Hemicraniectomy for massive middle cerebral artery territory infarction : a systematic review. Stroke. 2004; 35:539–543. PMID: 14707232.
Article10. Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, von Kummer R. 'Malignant' middle cerebral artery territory infarction : clinical course and prognostic signs. Arch Neurol. 1996; 53:309–315. PMID: 8929152.
Article11. Kirton A, deVeber G. Therapeutic approaches and advances in pediatric stroke. NeuroRx. 2006; 3:133–142. PMID: 16554252.
Article12. Lee MC, Frank JI, Kahana M, Tonsgard JH, Frim DM. Decompressive hemicraniectomy in a 6-year-old male after unilateral hemispheric stroke. Case report and review. Pediatr Neurosurg. 2003; 38:181–185. PMID: 12646736.
Article13. Lynch JK, Hirtz DG, DeVeber G, Nelson KB. Report of the National Institute of Neurological Disorders and Stroke workshop on perinatal and childhood stroke. Pediatrics. 2002; 109:116–123. PMID: 11773550.
Article14. Monagle P, Chan A, Massicotte P, Chalmers E, Michelson AD. Antithrombotic therapy in children : the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004; 126:645S–687S. PMID: 15383489.15. Murphy S. Deaths : final data for 1998. Natl Vital Stat Rep. 2000; 48:1–105. PMID: 10934859.16. Ng LK, Nimmannitya J. Massive cerebral infarction with severe brain swelling : a clinicopathological study. Stroke. 1970; 1:158–163. PMID: 5522913.
Article17. Ramaswamy V, Mehta V, Bauman M, Richer L, Massicotte P, Yager JY. Decompressive hemicraniectomy in children with severe ischemic stroke and life-threatening cerebral edema. J Child Neurol. 2008; 23:889–894. PMID: 18403586.
Article18. Rieke K, Schwab S, Krieger D, von Kummer R, Aschoff A, Schuchardt V, et al. Decompressive surgery in space-occupying hemispheric infarction : results of an open, prospective trial. Crit Care Med. 1995; 23:1576–1587. PMID: 7664561.19. Tan MA, Salonga AM, Jamora RD. Decompressive hemicraniectomy in a 2-year-old girl with a left middle cerebral artery infarct. Childs Nerv Syst. 2006; 22:523–525. PMID: 16328393.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effectiveness of Decompressive Craniectomy with Dural Augmentation in Malignant Cerebral Infarction
- Effects of Decompressive Craniectomy for the Management of Patients with Refractory Intracranial Hypertension
- Where are We Now with Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery Infarction?
- Therapeutic Hypothermia after Decompressive Craniectomy in Malignant Cerebral Infarction
- Surgical Management of Acute Infarction
