Dysphagia Caused by Osteochondroma of the Cervical Vertebral Body: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul Medical Center, Seoul, Korea. rocket-jinsoo@hanmail.net
- KMID: 1438407
- DOI: http://doi.org/10.5292/jkbjts.2012.18.1.32
Abstract
- A 56 year-old female presented with dysphagia 8 weeks ago and newly developed dysphonia 2 weeks ago. The radiology study and swallowing difficulty evaluation study revealed the esophagus and the posterior wall of the laryngopharynx to be severely compressed by the mass of the anterior 4th and 5th vertebral body of cervical spine. En bloc excisional biopsy of the bony mass was performed, which completely resolved the clinical symptoms. We report a rare case of osteochondroma occurring at the anterior portion of cervical spine leading to dysphasia and dysphonia with a review of relevant literature.
Keyword
MeSH Terms
Figure
-
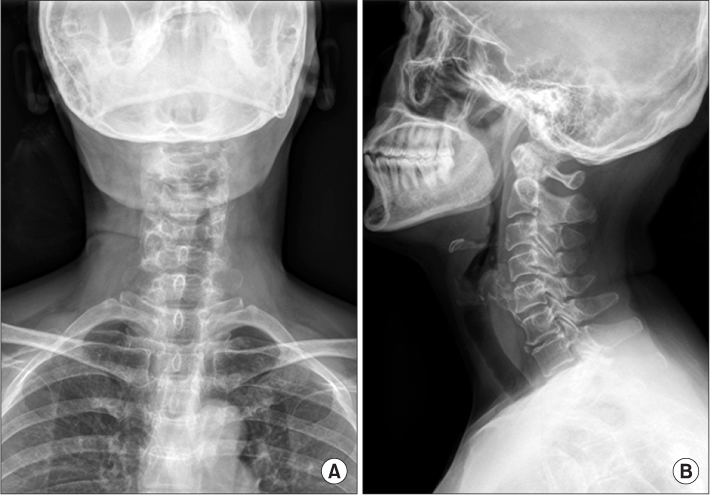
Figure 1 Radiographs of the cervical spine, anteroposterior (A) and lateral (B) view shows sclerotic and amorphous bony mass contained irregular bony trabeculae in the anterior 4th and 5th vertebral body of cervical spine.

Figure 2 CT scan images, sagittal image (A) shows an ossification from the C4 level to C5 level. Axial image (B) shows that the mass was developed on vertebral body of the 5th cervical vertebrae.

Figure 3 (A) Preoperative Gd-enhanced sagittal MRI demonstrated that the mass shows high signal intensity on C4-5 level. (B) Low signal intensity change of C4-5 mass shows on T2-weighted sagittal MRI. (C) Preoperative Gd-enhanced axial MRI of C3-4 mass shows heterogeneous signal intensity.

Figure 4 Photograph of excised tumor shows about 1.3×2.5×4.0 cm sized mass covering with cartilage layer.

Figure 5 Histopathologic examination shows the mature bone covered by a well differentiated cartilaginous cap (H&E, ×12.5).

Figure 6 Postoperative radiographs of the cervical spine, anteroposterior (A) and lateral (B) view shows removal of entire bony mass on vertebral body of the 5th cervical vertebrae.
Reference
-
1. Albrecht S, Crutchfield JS, SeGall GK. On spinal osteochondromas. J Neurosurg. 1992. 77:247–252.2. D'Ambrosia R, Ferguson AB Jr. The formation of osteochondroma by epiphyseal cartilage transplantation. Clin Orthop Relat Res. 1968. 61:103–115.3. Wang V, Chou D. Anterior C1-2 osteochondroma presenting with dysphagia and sleep apnea. J Clin Neurosci. 2009. 16:581–582.4. Mirra JM. Rosen G, editor. Benign cartilaginous exostoses. Bone tumors. 1989. 1st ed. California: Lea & Febiger.5. D'Ambrosia R, Ferguson AB Jr. The formation of osteochondroma by epiphyseal cartilage transplantation. Clin Orthop Relat Res. 1968. 61:103–115.6. Lee CJ, Cho WH, Chang HG, Choi SJ, Ha JO. Osteochondroma of the sacrum. J Korean Orthop Assoc. 1994. 29:314–317.7. Grivas TB, Polyzois VD, Xarchas K, Liapi G, Korres D. Seventh cervical vertebral body solitary osteochondroma. Report of a case and review of the literature. Eur Spine J. 2005. 14:795–798.8. Yim SJ, Kim YI, Choi CU. A case of osteochondroma which arised form right side lamina of 5th lumbar vertebra. J Korean Orthop Assoc. 1990. 25:597–601.9. Bernard SA, Murphey MD, Flemming DJ, Kransdorf MJ. Improved differentiation of benign osteochondromas from secondary chondrosarcomas with standardized measurement of cartilage cap at CT and MR imaging. Radiology. 2010. 255:857–865.10. Cho HM, Rhee SK, Kang YK, et al. Secondary Chondrosarcoma Arising from Osteochondroma(tosis). J Korean Bone Joint Tumor Soc. 2010. 16:21–26.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Williams Syndrome with Multiple Cervical Vertebral Fusion Presenting Dysphagia: A Case Report
- Cervical Cord Injury Associated with Osteochondroma Involving Cervical Lamina: Case Report
- Solitary Osteochondroma of the Atlas with Cervical Cord Compresion: Case Report
- Osteochondroma of the Cervical Spine: A Case Report
- Osteochondroma of the 5th and 6th Cervical Vertebral Body: One Case Report
