Korean Circ J.
2012 Jun;42(6):423-426. 10.4070/kcj.2012.42.6.423.
Extracorporeal Life Support After Prolonged Resuscitation for In-Hospital Cardiac Arrest due to Refractory Ventricular Fibrillation: Two Cases Resulting in a Full Recovery
- Affiliations
-
- 1Department of Internal Medicine, Soonchunhyang University Hospital, Seoul, Korea. jjw25@schmc.ac.kr
- 2Department of Chest Surgery, Soonchunhyang University Hospital, Seoul, Korea.
- KMID: 1433863
- DOI: http://doi.org/10.4070/kcj.2012.42.6.423
Abstract
- Extracorporeal life support (ECLS) has well demonstrated its efficacy in treating in-hospital cardiac arrest and is being used for broader indications. However, ECLS after prolonged cardiopulmonary resuscitation (CPR) has been traditionally contraindicated and is now challenging. Here, we introduce two cases of successful ECLS after prolonged CPR, resulting in a immediate and full recovery. Both these acute ST elevation myocardial infarction patients waiting for primary percutaneous coronary intervention (PCI) suddenly collapsed due to ventricular fibrillation (VF), which was refractory to conventional treatment. After 2 hours of conventional CPR, the ECLS had been implemented and primary PCI could be performed. Subsequent to successful revascularization, the VF was stopped with a single electric shock. In our second case, normal sinus rhythm was spontaneously restored after ECLS implementation, which was completed after 45 minutes of conventional resuscitation. Both patients made a full neurological recovery on the day of the event and were discharged with only minor complications.
MeSH Terms
Figure
-
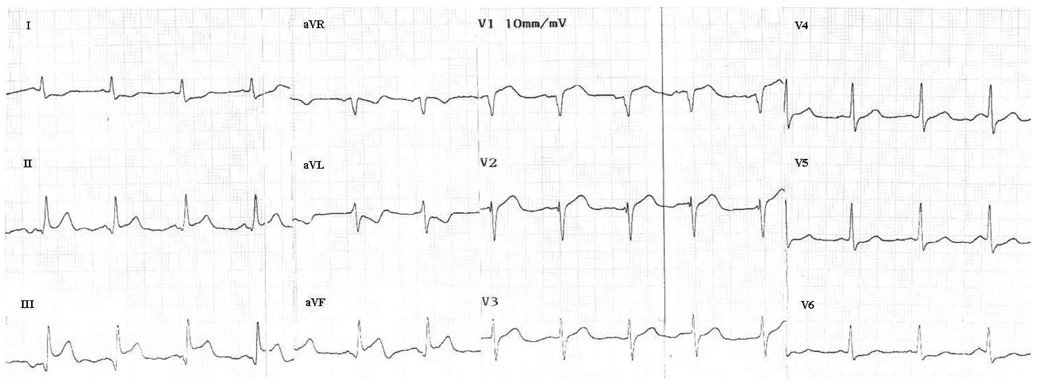
Fig. 1 Initial electrocardiogram (case 1).

Fig. 2 Ventricular fibrillation refractory to defibrillation (case 1).
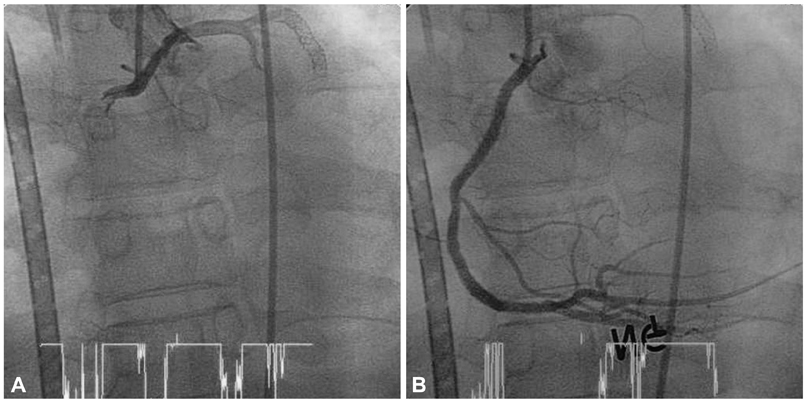
Fig. 3 Right coronary angiogram before (A) and after (B) primary percutaneous coronary intervention (case 1).
Cited by 1 articles
-
Cardiopulmonary resuscitation update
Sung Oh Hwang
J Korean Med Assoc. 2013;56(7):600-608. doi: 10.5124/jkma.2013.56.7.600.
Reference
-
1. Mehta RH, Starr AZ, Lopes RD, et al. Incidence of and outcomes associated with ventricular tachycardia or fibrillation in patients undergoing primary percutaneous coronary intervention. JAMA. 2009. 301:1779–1789.2. Chen YS, Lin JW, Yu HY, et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: an observational study and propensity analysis. Lancet. 2008. 372:554–561.3. Kurusz M, Zwischenberger JB. Percutaneous cardiopulmonary bypass for cardiac emergencies. Perfusion. 2002. 17:269–277.4. Rhee I, Gwon HC, Choi J, et al. Percutaneous cardiopulmonary support for emergency in-hospital cardiac arrest or cardiogenic shock. Korean Circ J. 2006. 36:11–16.5. Ramaraj R, Ewy GA. Rationale for continuous chest compression cardiopulmonary resuscitation. Heart. 2009. 95:1978–1982.6. Ong ME, Ng FS, Anushia P, et al. Comparison of chest compression only and standard cardiopulmonary resuscitation for out-of-hospital cardiac arrest in Singapore. Resuscitation. 2008. 78:119–126.7. SOS-KANTO study group. Cardiopulmonary resuscitation by bystanders with chest compression only (SOS-KANTO): an observational study. Lancet. 2007. 369:920–926.8. Ristagno G, Gullo A, Tang W, Weil MH. New cardiopulmonary resuscitation guidelines 2005: importance of uninterrupted chest compression. Crit Care Clin. 2006. 22:531–538.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Complete Recovery after Prolonged Resuscitation Using Extracorporeal Membrane Oxygenation for In-hospital Arrest Due to Refractory Ventricular Fibrillation
- Advanced Cardiac Life Support for Hyperkalemic Cardiac Arrest
- Recovery from Cardiac Arrest due to Ventricular Fibrillation: a case report
- Outcome of Resuscitation Attempts in Victims with Non Traumatic Out-of-Hospital Cardiac Arrest
- Successful resuscitation of refractory ventricular fibrillation with double sequence defibrillation
