J Korean Assoc Pediatr Surg.
2012 Dec;18(2):68-74. 10.13029/jkaps.2012.18.2.68.
Clinical Experience with Colonic Atresia
- Affiliations
-
- 1Division of Pediatric Surgery, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. sckim@amc.seoul.kr
- 2Division of Pediatric Surgery, GangNeung Asan Hospital, GangNeung, Korea.
- KMID: 1427993
- DOI: http://doi.org/10.13029/jkaps.2012.18.2.68
Abstract
- Colonic atresia (CA) is the rare cause of intestinal obstruction, and diagnosis of CA is difficult. But only few research has been performed, so little information has been available. The purposes of this study was to analyze the clinical findings of CA so that help physicians make decision properly. Children with CA who were treated at the division of pediatric surgery at Asan Medical Center in the period from January 1989 to December 2011 were evaluated retrospectively. A total of 6 children were treated with CA. These accounted for 2.7% of all gastrointestinal atresias managed in Asan Medical Center. Only one child was premature and low birth weight, the others were fullterm neonates and showed normal birth weight. Vomiting and abdominal distension were common symptoms and simple X-ray and barium study were used for diagnose of CA. But only 66.7% of the babies were diagnosed as CA pre-operatively. And 2 children out of 6 underwent re-operation due to missed CA at the time of the first operation. In aspect of types of atresia, the type IIIa were two, type IV were two, type I was one case, and one child showed rectal stenosis due to rectal web. Various operations were done according to individual findings and associated diseases. The 50% (n=3) of children underwent the primary anastomosis and the others (n=3) underwent colostomy first and staged operation later for missed CA or associated disease. All of them were recovered any significant complications. Therefore, the prognosis of CA is satisfactory if diagnosis and surgical management could be made properly. But because of the low incidence of CA, delay of diagnosis and treatment may occur. To prevent delay of diagnosis, we suggest prompt evaluation of doubtful infant and careful inspection of distal patency of bowel including whole colon and rectum when operating patients with intestinal atresia at any level.
MeSH Terms
Figure
-

Fig. 1 Image of simple X-ray at the age of 8days (Case No. 3).
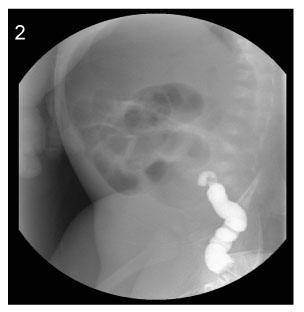
Fig. 2 Image of barium enema at the age of 8days (Case No. 3). The contrast cannot advance further.

Fig. 3 Image of simple X-ray at the age of 43days (Case No. 4).

Fig. 4 Image of barium enema at the age of 43days (Case No. 4). The contrast cannot advance further.

Fig. 5 Image of barium enema at the age of 5years (Case No. 6).
Reference
-
1. Powell RW, Raffensperger JG. Congenital colonic atresia. J Pediatr Surg. 1982. 17:166–170.2. Grosfeld JL, Ballantine TV, Shoemaker R. Operative management of intestinal atresia and stenosis based on pathologic findings. J Pediatr Surg. 1979. 14:368–375.3. Sturim HS, Ternberg JL. Congenital atresia of the colon. Surgery. 1966. 59:458–464.4. Davenport M, Bianchi A, Doig CM, et al. Colonic atresia: current results of treatment. J R Coll Surg Edinb. 1990. 35:25–28.5. Black PR, Mueller D, Crow J, et al. Mesenteric defects as a cause of intestinal volvulus without malrotation and as the possible primary etiology of intestinal atresia. J Pediatr Surg. 1994. 29:1339–1343.6. Coran AG, Eraklis AJ. Atresia of the colon. Surgery. 1969. 65:828–831.7. Ogunyemi D. Gastroschisis complicated by midgut atresia, absorption of bowel, and closure of the abdominal wall defect. Fetal Diagn Ther. 2001. 16:227–230.8. Ashburn DA, Pranikoff T, Turner CS. Unusual presentations of gastroschisis. Am Surg. 2002. 68:724–727.9. Basaran UN, Inan M, Gucer F, et al. Prenatally closed gastroschisis with midgut atresia. Pediatr Surg Int. 2002. 18:550–552.10. Al Wafi A, Morris-Stiff G, Lari A. Colonic atresia secondary to a choledochal cyst. Pediatr Surg Int. 1998. 13:422–423.11. Erskine JM. Colonic stenosis in the newborn: the possible thromboembolic etiology of intestinal stenosis and atresia. J Pediatr Surg. 1970. 5:321–333.12. Alexander I. Congenital varicella. BMJ. 1979. 2:1074.13. Hitchcock R, Birthistle K, Carrington D, et al. Colonic atresia and spinal cord atrophy associated with a case of fetal varicella syndrome. J Pediatr Surg. 1995. 30:1344–1347.14. Sauve RS, Leung AK. Congenital varicella syndrome with colonic atresias. Clin Pediatr (Phila). 2003. 42:451–453.15. Grosfeld JL, Ballantine TV, Shoemaker R. Operative management of intestinal atresia and stenosis based on pathologic findings. J Pediatr Surg. 1979. 14:368–375.16. Rescorla FJ, Grosfeld JL. Intestinal atresia and stenosis: analysis of survival in 120 cases. Surgery. 1985. 98:668–676.17. Dalla Vecchia LK, Grosfeld JL, West KW, et al. Intestinal atresia and stenosis: a 25-year experience with 277 cases. Arch Surg. 1998. 133:490–496.18. Barlas E, Gunyuz T. Atresia of the colon. J Pediatr Surg. 2005. 40:1258–1268.19. Ibrahim K. Colonic atresia: surgical management of outcome. Pediatr Surg Int. 2001. 17:631–635.20. Kim SC, Kim DY, Kim SY, Kim IK, Kim IS, Kim JE, Kim JC, Kim HY, Park KW, Park WH, Park JY, Seo JM, Seol JY, Oh SM, Oh JT, Lee NH, Lee MD, Lee SK, Lee SC, Chung SY, Jung SE, Jeong YJ, Jung PM, Choi KJ, Choi SJ, Choi SO, Choi SH, Choi YM, Han SJ, Hong J. Intestinal atresia-The second national survey. J Korean Assoc Pediatr Surg. 2010. 16:1–10.21. Freeman NV. Congenital atresia and stenosis of the colon. Br J Surg. 1966. 53:595–599.22. Coran AG, Eraklis AJ. Atresia of the colon. Surgery. 1969. 65:828–831.23. Schiller M, Aviad I, Freund H. Congenital colonic atresia and stenosis. Am J Surg. 1979. 138:721–724.24. Boles ET Jr, Vassy LE, Ralston M. Atresia of the colon. J Pediatr Surg. 1976. 11:69–75.25. Watts AC, Sabharwal AJ, MacKinlay GA. Congenital colonic atresia: should primary anastomosis always be the goal? Pediatr Surg Int. 2003. 19:14–17.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of Down syndrome associated with colonic atresia
- Colonic Web Associatd with Imperforate Anus
- A Case of Congenital Colonic Atresia Associated with Imperforate Anus
- Radiologic Evaluation of Intestinal Obstruction in the Neonates
- Esophageal Atresia with Tracheoesophageal Fistula: Clinical experience of 20 cases
